|
Read time: 15 min
|
Posted on:
Most telehealth visits are over in five minutes. Dr. Vijaya Galic’s visits tend to run fifteen or twenty, and for her, that difference is the entire point.
Before she retired, Dr. Galic spent her career as a gynecologic oncologist, performing some of the most complex cancer surgeries in her field and training the next generation of doctors as a teacher and faculty member. That background shaped a simple conviction she now brings to every virtual visit: you don’t want to mistake convenience for correctness.
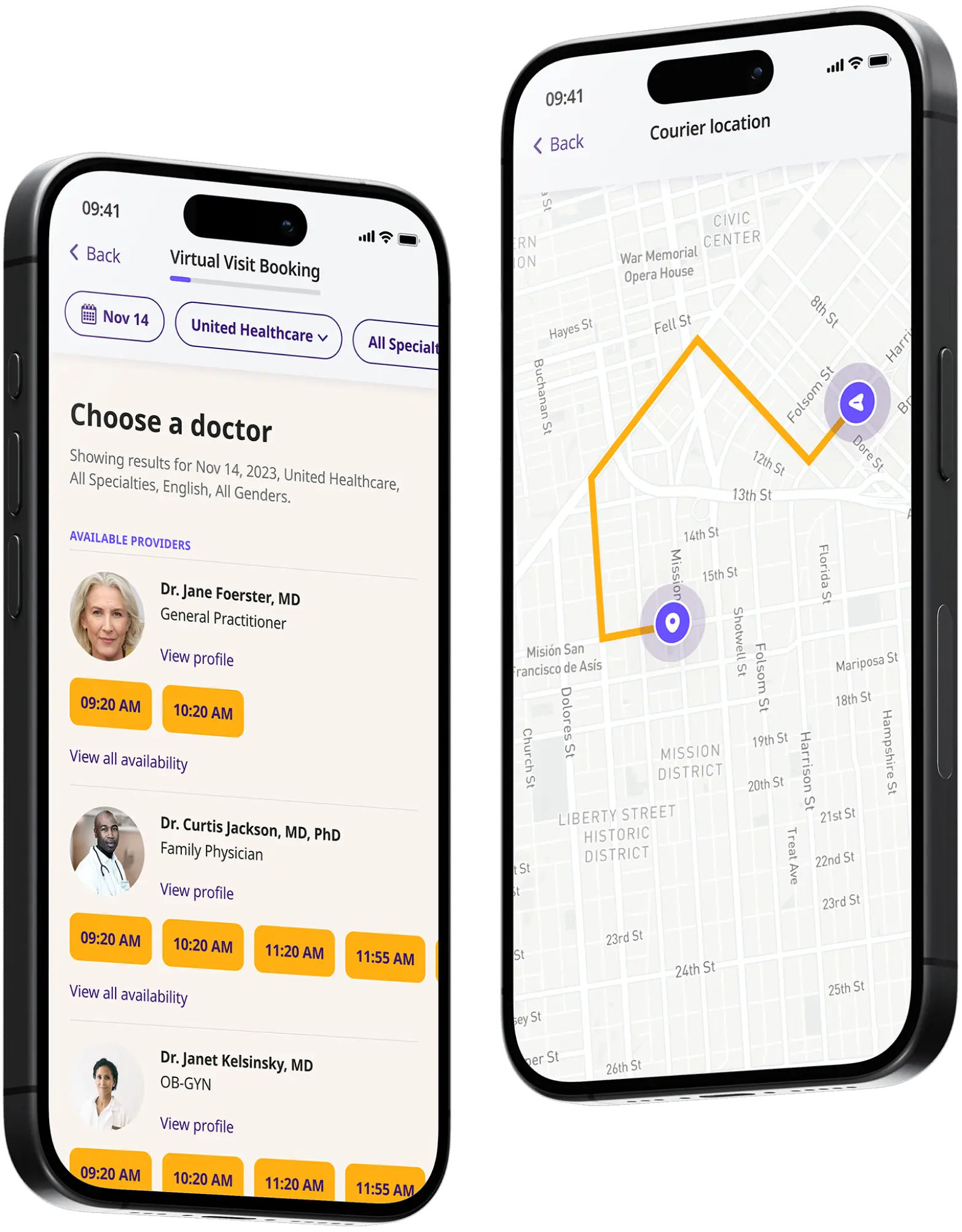
Today she sees patients on DrHouse the same way she ran her in-person practice, ordering labs and imaging, making referrals, and following up on results herself. But she isn’t just transplanting an old practice online.
She’s actively pushing at what telehealth can do, coaching patients to send her photos and at-home readings, using the platform’s messaging and lab tools, and taking on complex cases that most virtual visits would never touch.
In this interview, Dr. Galic shares her unconventional path into medicine, why she traded the operating room for telehealth, the kinds of cases she manages remotely, and how she keeps finding new ways to do more from a distance.

Dr. Vijaya Galic is a board-certified physician whose primary specialty, before retiring from surgery, was gynecologic oncology, a separate board-certified field from OB-GYN focused on caring for women with cancer. Her work spanned chemotherapy, radical surgery across the chest, abdomen, and pelvis, reconstructive urology, and end-of-life care.
Over her career she built and led complex surgical programs, including hyperthermic chemotherapy and transfusion-free surgery, and specialized in rare, ultra-radical operations that very few surgeons perform.
She was also a longtime educator, training fellows, residents, and medical students, serving on faculty, and teaching board exam courses. After decades in academic and clinical medicine, she retired from the operating room and now practices full time through telehealth.
That depth of experience is why she’s comfortable treating almost anything that comes through a virtual visit, with one exception she’s happy to name.
Her approach reflects a particular philosophy: that virtual care, done properly, doesn’t have to mean cutting corners.
We spoke with Dr. Galic about her background, how she practices, and what she wants patients to understand about getting real medical care online. Below, she shares her perspective in her own words.
I’m listed technically as an OB-GYN, which is not incorrect. But my real specialty before I retired was as a gynecologic oncologist. That’s a separate, board-certified specialty from OB-GYN, where I take care of women who have cancer, and that involves everything: chemotherapy, surgery, and not just pelvic surgery but chest, abdomen, pelvis, and end-of-life care. So that was my practice before I retired, which essentially qualifies me to do just about anything.
So when I decided to retire and came on to DrHouse, I essentially agreed to do just about anything, and I’m comfortable doing just about anything. I do not do medical weight loss, though. It’s the only thing I don’t do. But everything else is fair game.
I see men, I see women. I had a urology practice, so I do a lot of advanced urology. I can manage advanced gynecology and basic gynecology. If you show me a spot on your arm, I can probably help you figure out what it is, and if not, refer you. That’s kind of my experience in a nutshell.
On DrHouse, the most common condition I treat is actually urinary tract infections. Being essentially a reconstructive urologist, I can manage them very, very comprehensively, the recurrent ones, the complicated ones. Then I see lots and lots of things that aren’t right downstairs, and that’s both genders, things people feel uncomfortable bringing to their in-person doctor. I always tell people: I don’t judge, and I can fix most things.
It was really on a whim. My mother was a surgeon, she came to the US from India in 1969, set up practice, and was highly successful. I had other relatives who were physicians too. I was the black sheep. I was the rebel. I was that one cousin.
I had a dog kennel, I had farm animals, and I went to Cornell as a pre-vet, and I thought that was what I was going to do, but I kind of got bored. So I had to do some twenty-something finding-myself of sorts. I got an MBA, I was working in marketing, I was even bartending, which I think helps in some ways with certain types of patients.
I did this on a whim. I didn’t even have the prerequisites for medical school done. I picked them up in community college, took the MCAT in August, cobbled together an application, and tossed it out there. I got into the University of Washington, which was top ten at the time. It was one of those meant-to-be things. I didn’t fully understand what I was getting into.
While I was doing my MBA, I’d been working in a research lab at Hopkins, interacting with oncologists and people who treated ovarian cancer in very advanced ways, clinical trial leaders. I was meeting all the right people. I just didn’t realize the significance at the time, how they would play a role in my life later.
I knew I wanted to do cancer surgery, that I wanted to be some kind of oncologist. I relatively struggled on internal medicine, mostly because I didn’t have the patience to write all those notes. And when I went into my surgery rotation, I said, oh my God, I’m a surgeon. We were done rounding by 6:30, and our notes were three lines long. It’s awesome. This is for me. The path was somewhat winding, but here I am.
I previously had this retirement dream of one day opening a little travel medicine clinic in Hawaii. But because of certain lifestyle choices I have, like a dog kennel, that wasn’t feasible in the long run. However, telehealth has sort of enabled me to live my dream.
Before COVID, I could spend an hour on the phone getting a patient into the hospital or the ER, and we wouldn’t get paid for it. What COVID did was equalize reimbursements for telehealth and make it a viable venue for patients. And we learned that we didn’t have to bring everybody into the office. Now telehealth is here to stay, it’s advancing in technology, and it’s incredibly convenient for patients.
I keep my schedule open from about 6 a.m. until 10 p.m. my time, because I’m running my retirement dog kennel and I have to be awake and here anyway. So I might as well help out that patient who has a UTI, burning when they pee, at nine o’clock at night on a Sunday.
After working multiple telehealth platforms, I can tell you DrHouse is by far the most robust. I’ve almost replicated my office. I can order imaging, I can order labs, I can refer patients. I can almost function like their primary care doctor. My support staff is amazing, the most wonderful people. Out of every platform I’ve worked on, this one is extremely viable and full-service.
I actually quit my other telehealth platform to do DrHouse full time.
The thing I would probably cross-stitch is this: you don’t want to mistake convenience for correctness.
When I did my OB-GYN residency, I knew I was going into gyn-onc, and I knew I had to be top, top. In gynecology, people live and die by your correctness, your following of the data, your adherence to guidelines. So that’s very deeply ingrained in me. And when I got to telehealth, the patients want convenience, and sometimes the easy way out is not the right way.
The average telehealth visit will often span five minutes. Mine average probably fifteen to twenty. When I see a UTI patient, I explain that it’ll be exactly like you came into my office. That disclaimer at the bottom that says if your antibiotic fails, go to the ER, that doesn’t apply, because I would never say that to somebody who came to my office. But it means that you, the patient, have to partner in your care. You’ll receive a lab slip for a urine culture, and I will follow up that result for you. We work together, and we solve it, without you going into an urgent care or going to the ER. But you have to come to the table prepared to participate.
I practice antibiotic stewardship, and it’s not just a blurb. People are so cavalier about taking antibiotics, and they don’t understand the damage they’re doing to themselves. So I’d rather take the time and not shortcut. I wanted to change the format of my practice, but I didn’t want to make my practice substandard.
A lot of what I see, people haven’t been able to solve elsewhere. I flat out tell them I’m not God or magic, but I do have a really good command of data, and I keep access to all of the resources I had as an oncologist for managing really complex medical patients. So I can use those resources to help patients here.
Urinary tract infections are my most common diagnosis, and I manage them the way a urology practice would. I had a lady with ten documented UTIs in a year. Anything more than three, I’m sending people to urology for a workup. The kidney is a wall socket to the bloodstream, so I take these seriously, I’ve seen people end up in the ICU, go uroseptic. I have young patients, twenty-one, twenty-two, with multi-drug-resistant UTIs. One I had to set up for IV antibiotics for a week, because that was the last and only thing her bacteria would respond to.
I also see things people simply hadn’t connected. I had a patient with known herpes who came in with severe jaw and head pain, so bad she couldn’t open her mouth. She had classic trigeminal neuralgia. I put her on high-dose Tegretol, and at her follow-up she wanted to show me that she could eat again and her pain was almost gone.
Hormones are another big one. Endocrinology is its own complex specialty, and a lot of the people running online hormone mills aren’t endocrinologists. As an oncologist, I treated cancers that resulted from mismanaged hormone use, so I’m extremely particular. I call it no-nonsense HRT, done by the guidelines.
And then there’s triage. When something needs in-person care, I treat it exactly like I would from my office. I write a note that itemizes what I’m requesting, labs, IV antibiotics, a specific medication to consider, so the patient isn’t just showing up at the ER unable to tell the story. I once caught a patient on a dangerous drug-disease combination, a heart rhythm condition paired with a medication that makes it worse, and sent her in with a full list of what needed to be checked. I run interaction software on every prescription, because the goal is to never let the holes line up like Swiss cheese.
If I can see it, I can treat it, so a lot of what excites me is figuring out how to see more. The Amazon otoscope is thirty bucks, and now patients are sending me ear photos all the time. I tell everyone with kids to just go buy one, kids get ear infections constantly, take a look, send a photo to the doc. Patients with the right phones can even send me pulse oximetry readings or EKGs.
The platform keeps growing with me. First we could just do labs. Then imaging. Now patients can message me, they’ll even write something on paper, take a photo, and upload it to their chart, and I can respond. I had a patient with cellulitis outline the red area with a Sharpie so we could track whether it was spreading, and she sent me photos as it went. My frequent patients have standing lab orders, so at the first sign of a UTI they can just go drop a specimen and I’ll see the result.
I’m also able to send people for self-collect swabs at the lab, which means I can screen for things like HPV without the patient ever sitting in a waiting room. And I keep a wish list, right now I’m working with one of the labs to figure out how to get strep testing on the platform. There’s always something I’m trying to add.
Educating them. I’ve trained fellows, residents, and medical students, I’ve been faculty, I taught board exam courses, so teaching is just part of who I am. With patients, I enjoy explaining things and answering their questions, and with the new messaging feature, if we run out of time during a visit, I’ll just tell them to message me and we’ll finish it.
All of my patients get handouts, and these aren’t just any handouts. They come from a clinical decision tool we use in hospitals called UpToDate, all peer-reviewed literature, reviewed and updated every six months by experts in the field. So when I hand something to a patient, I can tell them it’s based on data, not on whatever they happened to find online. That matters to me.
Probably the dog kennel. I run a sixty-dog kennel as my retirement, and right now I have about four litters upstairs, with some foster moms raising the ones whose own mothers aren’t as good at it. I have dogs from all over, one from Lithuania, one from Bulgaria who came over with no manners whatsoever, one from China, a Canadian. I even have a little one who lives right in my telemedicine station with me.
People are also sometimes surprised by my path. I didn’t take a straight line into medicine. I was a pre-vet with farm animals, then went into business and marketing, and even bartended for a while. I think all of those non-medical experiences have helped me connect a little better with people.
Don’t forget the basics. There’s so much marketing, and this desire to keep jumping to the new thing, that the basics are completely forgotten. People want to try out all these crazy supplements and spend crazy money, but they don’t want to eat real food.
I have people spending hundreds of dollars on urinary tract supplements, and the only thing that has data behind it is cranberry pills. Simple. So you don’t have to be model skinny, but a reasonable weight. That old saying holds: moderation, moderation. And if you get on one of my visits and you start vaping, I’m going to yell at you, just so you know.
I’m also a little concerned with any sort of drug that requires a lifetime commitment. I always do it safely. That’s kind of how I do everything.
For Dr. Galic, telehealth isn’t a lighter version of medicine. It’s the same rigorous practice she built over a career in cancer care and teaching, delivered in a more accessible form. She listens longer, asks more, orders the tests, follows up on the results, educates at every step, and keeps finding new ways to do more from a distance.
Whether she’s untangling a case no one else could solve, catching something that’s been missed, or simply talking a patient through the basics, her goal stays the same: bring the full weight of her experience to every visit, and treat each patient as a partner in their own care.
Dr. Galic is currently seeing patients through virtual visits on DrHouse, continuing the work she’s done throughout her career while making thorough, by-the-book care available wherever her patients are.
Content on the DrHouse website is written by our medical content team and reviewed by qualified MDs, PhDs, NPs, and PharmDs. We follow strict content creation guidelines to ensure accurate medical information. However, this content is for informational purposes only and not a substitute for professional medical advice, diagnosis, or treatment. For more information read our medical disclaimer.
Always consult with your physician or other qualified health providers about medical concerns. Never disregard professional medical advice or delay seeking it based on what you read on this website.
If you are experiencing high fever (>103F/39.4C), shortness of breath, difficulty breathing, chest pain, heart palpitations, abnormal bruising, abnormal bleeding, extreme fatigue, dizziness, new weakness or paralysis, difficulty with speech, confusion, extreme pain in any body part, or inability to remain hydrated or keep down fluids or feel you may have any other life-threatening condition, please go to the emergency department or call 911 immediately.
Experience 24/7 complete care in one visit, including treatment, prescriptions, and delivery.









on your schedule
Skip the unnecessary waiting room,
see a board-certified clinician now.
Prescriptions as needed
Renew or get a new Rx.
On-demand virtual visits
See a physician 24/7.
24/7 care support
We are here to help you.
Download the DrHouse app.
Set up your free account in a minute.
Start a visit with an online doctor. Wait time is less than 15 minutes.
Get an Rx from your preferred pharmacy. Pick up a Rx nearby or get it delivered to you.

on your schedule
Skip the unnecessary waiting room, see a board-certified physician now.
Available in 50 states. Insurance accepted.