|
Read time: 14 min
|
Posted on:
A few years ago, an AI that could answer the phone, understand a worried parent describing a child’s fever, and book the right appointment was science fiction. In 2026 it is something you can buy, and vendors are selling it hard, promising your clinic will never miss another call.
So the honest question for a practice owner is not really “can AI answer the phone.” It can, and it does it well.
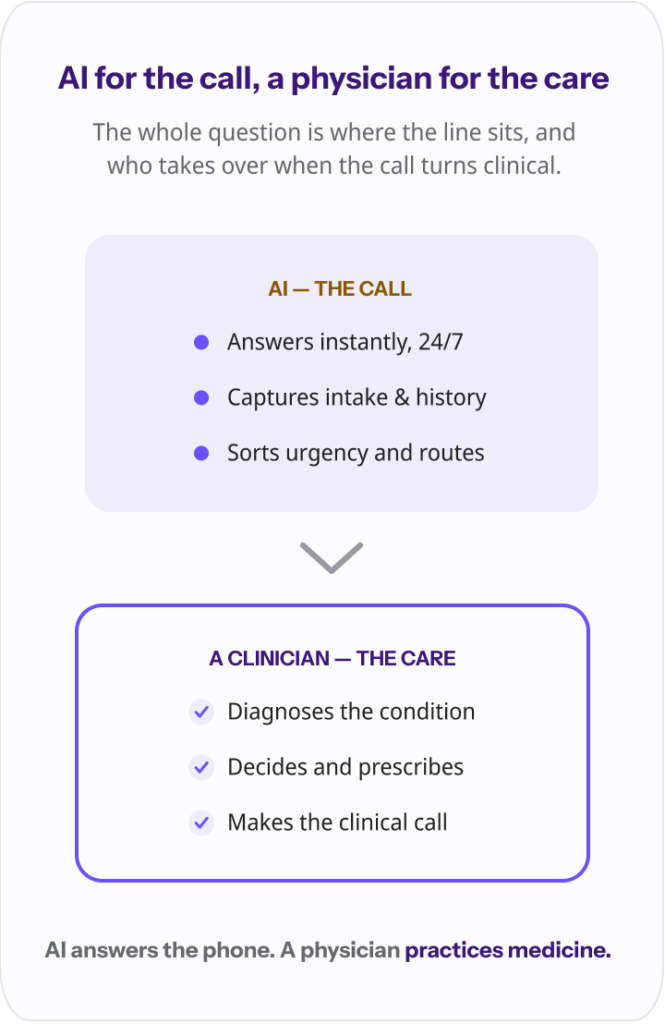
The question is how much of a sick patient’s after-hours call an AI should handle, and who takes over when the call stops being about scheduling and starts being about symptoms. That line is the whole story, and getting it right is the difference between a system that helps your patients and one that quietly puts them at risk.
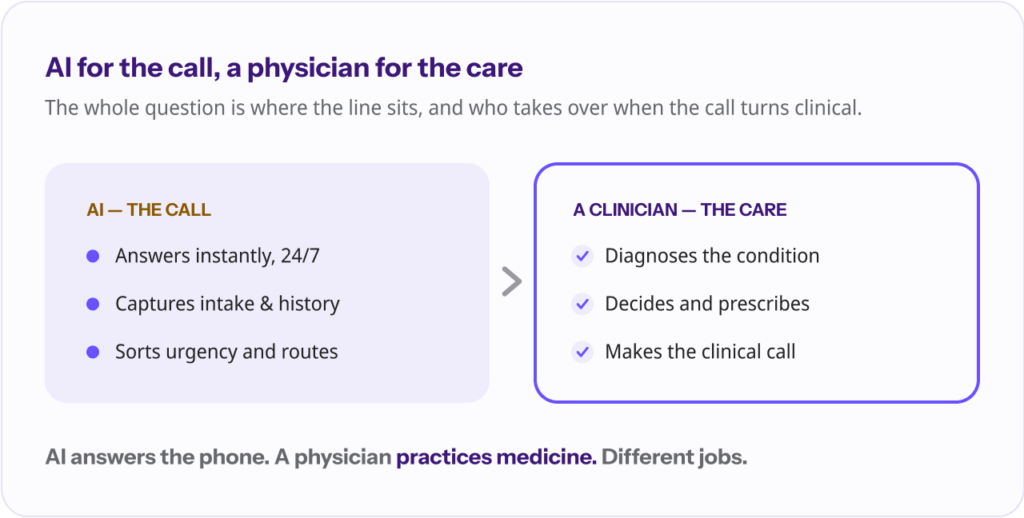
The short version: Yes, and no. AI can reliably answer after-hours calls, capture intake, sort urgency, and route or escalate, and for those jobs it is genuinely good and getting better fast. What AI cannot safely do is make the clinical decision: diagnose, treat, or stand in for a clinician. The workable model is AI for the call, a human for the care.
Start with the good news, because it is real. Modern voice AI has crossed a threshold. It answers on the first ring, at 2 a.m., on a holiday, with no hold music and no voicemail. For the routine and administrative bulk of after-hours calls, it is a genuine upgrade over the alternatives.
Specifically, today’s systems handle the front of the call well: greeting the patient and answering in natural language, capturing intake and history, collecting and structuring a patient’s symptoms, assessing urgency to sort and route the call, scheduling appointments and taking refill requests, documenting the interaction into a summary for the practice, and flagging or escalating anything that needs a person.
This is not hype, and physicians are not standing on the sidelines. In the American Medical Association’s 2026 survey of roughly 1,700 doctors, 81% reported using AI in their practice, more than double the 38% who did in 2023. More than three-quarters said AI improves their ability to care for patients, up from 65% two years earlier, and the most common uses are exactly the unglamorous administrative ones: documentation and summarization.
AI is good at the paperwork around care, and clinicians have noticed.
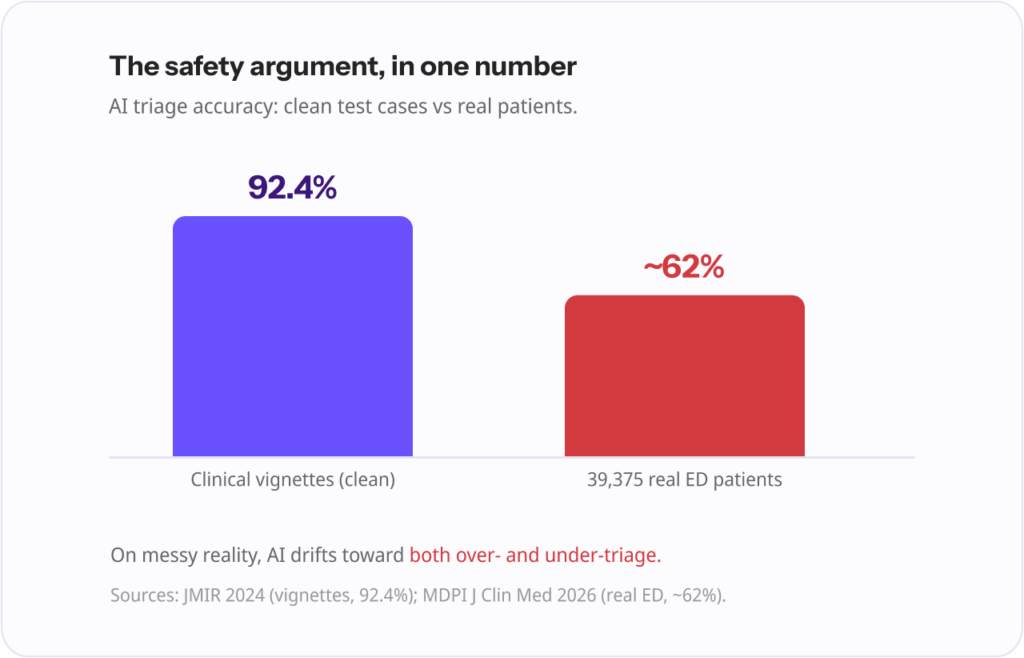
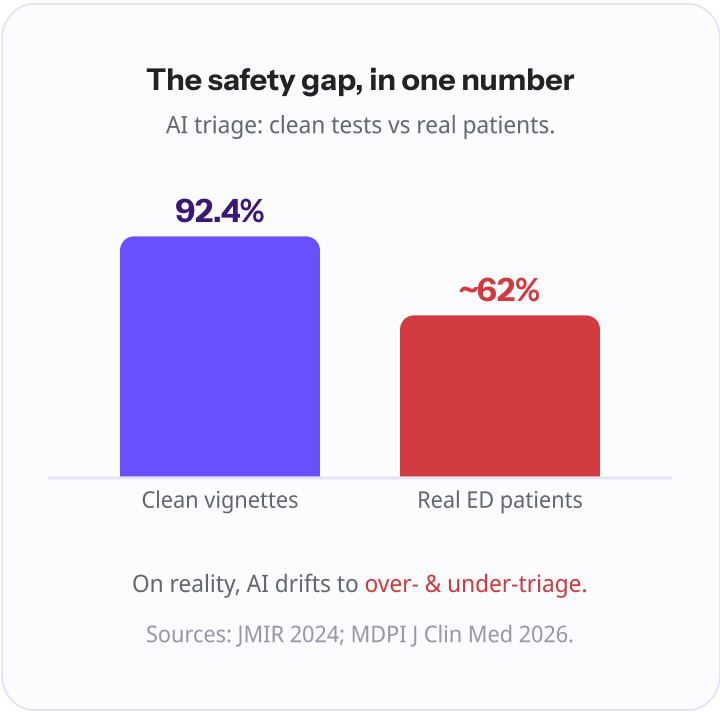
It is even capable at the triage-sorting task itself, in the right conditions. When researchers tested frontier models on standardized clinical vignettes, the AI triaged them at 92.4% accuracy, essentially matching primary care physicians at 91.3% and far ahead of laypeople using an internet search. Only two years earlier, an older model had been significantly worse than physicians at the same task. The trajectory is steep.
If the job is answering the phone and getting the patient to the right place, AI is ready. The problem starts when we ask it to do the next thing.
Here is the line, and it matters more than any feature list: AI should not assess symptoms in order to make a clinical decision, diagnose a condition, recommend treatment, or stand in for the clinician. Not because the technology is useless, but because the stakes and the evidence say so.
Those impressive vignette scores come with a catch. Clinical vignettes are clean and complete. Real patients calling at night are not. When the same kind of models were tested against a real emergency dataset of 39,375 patients, the best of them agreed with physician triage only about 62% of the time, and the study found the models drifted toward both over-triage and under-triage.
A broader meta-analysis of 50 studies across 25 different models found performance promising but highly variable depending on the model and the task. The gap between 92% on tidy vignettes and 62% on messy reality is the entire safety argument in one number.
There is a second problem specific to how these systems work. Large language models can produce “hallucinations”, answers that are fluent, confident, and completely wrong. A scoping review of AI in emergency triage put it plainly: the technology shows promise, but overconfident answers may present real dangers to patients, and safe deployment requires human oversight and validation.
A wrong answer delivered with total confidence at 2 a.m., with no clinician in the loop, is exactly the failure mode you cannot accept in medicine.
And some calls simply need a person regardless of accuracy: the frightened patient, the one in crisis, the situation that does not fit any protocol. Empathy and judgment are not features you configure.
“AI is genuinely excellent at the front of the call. It answers on the first ring, it never sleeps, it captures the intake cleanly, and it gets the patient to the right place. The mistake is letting it keep going and pretend to be the doctor. Answering the phone and practicing medicine are not the same job, and the safe systems know exactly where one ends and the other begins.” Ergo Sooru, Co-Founder & CEO, DrHouse
| AI handles this well | This needs a human clinician |
|---|---|
| Answering instantly, 24/7, with no hold | Diagnosing a condition |
| Capturing intake and patient history | Deciding on treatment |
| Collecting and structuring symptoms | Prescribing medication |
| Assessing urgency to sort and route | Making the final clinical judgment |
| Scheduling and taking refill requests | Handling an emotional or crisis call |
| Documenting and summarizing the call | Anything ambiguous or high-acuity |
| Recognizing and escalating urgent calls | Standing in for the clinician |
This split is not a knock on AI. It is how the credible systems are already designed. The best-known platforms use what the field calls deterministic guardrails: the AI answers routine questions and routes, and anything that crosses into clinical territory is escalated to a person rather than answered.
The consensus in the industry is not “AI or humans.” It is AI plus a human. Which raises the question almost nobody answers well.
Everyone agrees a human should make the clinical decision. The question is which human, and this is where most after-hours setups quietly fall short.
The default answer is “escalate to your own on-call provider.” That keeps care safe, but look at what it actually does: the AI takes the call, and then your own physician gets woken up to handle it. You have added software to the exact same burnout. The call is still landing on your team in the middle of the night.
The other common answer is a nurse advice line: the AI does intake, then a nurse assesses and advises where the patient should go. That is safer and useful, but a triage nurse advises and directs; they cannot diagnose or treat.
The patient’s problem is routed, not resolved, and often ends up back with your practice in the morning or at the urgent care down the street.
| Model | After-hours coverage | Does it resolve the case? | Burden on your team | Cost to the practice |
|---|---|---|---|---|
| AI only | 24/7 | No, unsafe to let AI decide | Low | Low |
| AI plus your on-call doctor | 24/7 intake | Yes, but your doctor is woken | High | Your staffing cost |
| AI plus a nurse advice line | 24/7 | No, advice only | Low | Per-call or subscription |
| AI plus physician coverage | 24/7 | Yes, treated | None | Can be $0 |
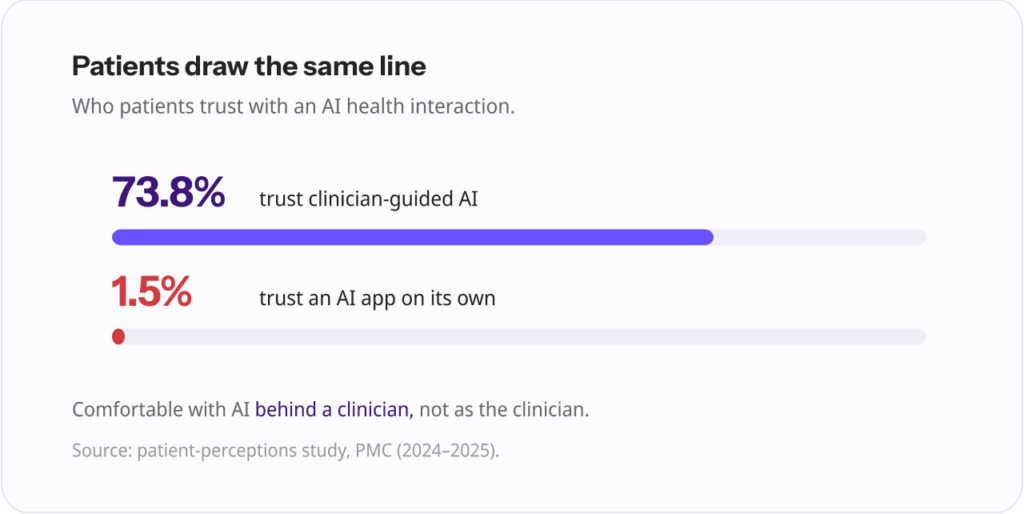
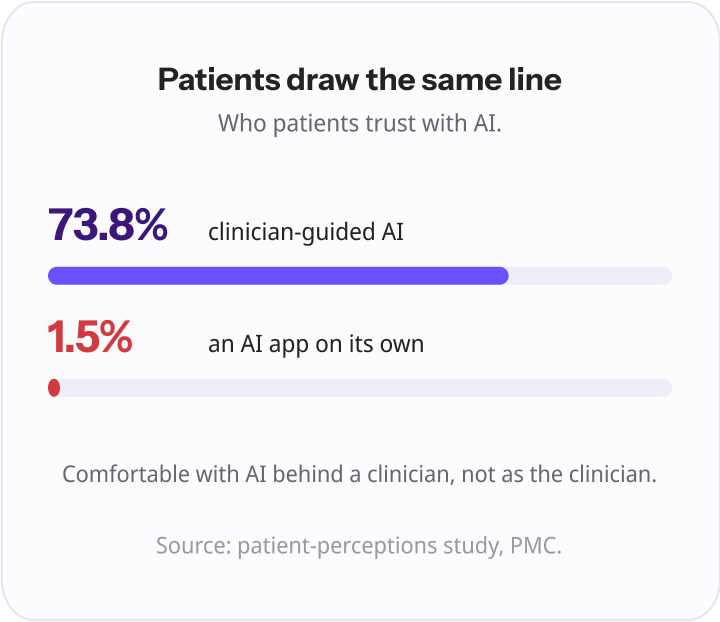
Patients feel this distinction too. In one study, 73.8% of patients trusted clinician-guided AI, while only 1.5% trusted an AI app on its own. People are comfortable with AI as long as a clinician is behind it. They are not comfortable with AI as the clinician, and they are right not to be.
“Everyone agrees a human should make the clinical decision. The question nobody answers well is which human. If the answer is ‘your own on-call doctor at 2 a.m.,’ you have not solved anything, you have just added software to the same burnout. The point of AI here is to hand the clinical part to a physician who can actually treat the patient, so your team can sleep.” Ergo Sooru, Co-Founder & CEO, DrHouse
Put the pieces together and the answer is straightforward. Use AI for what it is good at, and a physician for what only a clinician should do.
In practice that means the AI answers the after-hours call, captures intake, and triages and routes on your practice’s rules, without ever making a diagnosis or a treatment decision.
Then, for the eligible non-emergency cases, a board-certified physician takes over: evaluating the patient by video, treating the condition, and prescribing when clinically appropriate and subject to physician judgment, patient eligibility, and applicable state laws.
True emergencies are escalated, not handled by AI or by video. This is the design DrHouse uses, and the important detail is what the AI is and is not allowed to do: it handles intake and routing before a physician connects, and the clinical decision belongs to the physician.
The reason this beats the alternatives is that it removes the work instead of relocating it. Your own physicians are not paged. The patient is not merely told where to go; they are treated, and the case is resolved in a single contact, with notes routed back to your practice and the patient still attributed to you.
And a physician handling it is not the expensive luxury it sounds like: telemedicine visits averaged about $97 per episode of care versus roughly $509 for in-person in a large 2026 analysis. When the model is care-based, this can be offered at no cost to the practice at all.
When you evaluate any AI after-hours solution, these are the things that actually matter.
| What to look for | Why it matters |
|---|---|
| HIPAA compliance and clear data handling | You are trusting a vendor with protected health information |
| Guardrails and a real escalation pathway | Keeps AI in its lane and moves emergencies to a person fast |
| Documentation returned to your practice | Continuity; you know what happened overnight |
| Specialty-awareness | The right protocols and urgency thresholds for your practice |
| A clinical backstop that treats, not just advises | Determines whether calls get resolved or merely rerouted |
That last row is the one to weigh hardest. Everything above it is table stakes a competent vendor will meet. Whether there is a clinician who can actually treat the patient, and who that clinician is, decides whether your after-hours calls come back to you resolved or just come back to you.
You can see how this plays out in our comparison of physician-led after-hours coverage versus a message-and-triage line.
This is a topic full of reasonable skepticism, and it deserves straight answers.
No, and the framing is wrong. The AMA’s own position is that AI should enhance, not replace, clinicians, and the same logic applies to your front desk. AI offloads the repetitive intake and after-hours overflow so your people can focus on the patients in front of them, not the twentieth scheduling call of the hour.
They accept it for the right things. The evidence is that patients are comfortable with AI handling information and intake, and strongly prefer a clinician for anything clinical.
Physicians agree: in the AMA survey they were comfortable with patients using AI for medication and general health questions, but nearly half would not want AI interpreting pathology or radiology results. Used within its lane, AI does not erode trust; used beyond it, it does.
Only with the guardrails above: escalation, human oversight, and a clinical backstop. On its own, making decisions, it is not, and no responsible vendor claims otherwise.
Physicians ranked validated safety and efficacy and clear liability frameworks as their top prerequisites for trusting AI, and those are the right questions to ask any vendor.
The question was never really “can AI replace the after-hours call?” It was “which parts should AI handle, and who handles the rest?”
AI belongs at the front of the call, answering instantly, taking intake, sorting urgency, and getting the patient to the right place. It is good at that, and getting better. The clinical decision belongs to a clinician, because the evidence, and your patients, say so.
Get that division right and you give patients something they rarely get after hours: an instant answer and real care, without burning out your own team to provide it. That is the model worth looking for. AI for the call, a physician for the care.
Yes. Modern voice AI can answer after-hours and overflow calls instantly, capture intake, collect symptoms, assess urgency, schedule appointments, take refill requests, and document the call. It handles the administrative front of the call well.
AI can help sort urgency and route calls, and on clean test cases it approaches physician-level accuracy. But it cannot safely make a diagnosis or a treatment decision. On real patients, AI triage agreement with physicians drops significantly and can drift toward over- or under-triage, so a human clinician should make the clinical call.
It is safe for intake, routing, scheduling, and documentation when the system has proper guardrails and escalates anything clinical to a person. It is not safe to let AI make clinical decisions on its own. Look for HIPAA compliance, a clear escalation pathway, and a clinician backstop.
The mainstream view, including the AMA’s, is that AI should enhance rather than replace people. In practice it offloads repetitive intake and after-hours overflow so staff can focus on higher-value work, not that it removes the need for a team.
Pricing varies widely by model and features, from per-call or per-seat software to full managed services. The more important cost question is what happens after the AI answers: a model where a physician resolves the clinical cases can be offered at no cost to the practice when care is billed to the patient or insurance.
A well-designed system recognizes urgency signals and escalates immediately, to your on-call provider, to a covering physician, or to emergency services, rather than trying to handle it automatically. Escalation quality is one of the most important things to evaluate.
Content on the DrHouse website is written by our medical content team and reviewed by qualified MDs, PhDs, NPs, and PharmDs. We follow strict content creation guidelines to ensure accurate medical information. However, this content is for informational purposes only and not a substitute for professional medical advice, diagnosis, or treatment. For more information read our medical disclaimer.
Always consult with your physician or other qualified health providers about medical concerns. Never disregard professional medical advice or delay seeking it based on what you read on this website.
If you are experiencing high fever (>103F/39.4C), shortness of breath, difficulty breathing, chest pain, heart palpitations, abnormal bruising, abnormal bleeding, extreme fatigue, dizziness, new weakness or paralysis, difficulty with speech, confusion, extreme pain in any body part, or inability to remain hydrated or keep down fluids or feel you may have any other life-threatening condition, please go to the emergency department or call 911 immediately.
Experience 24/7 complete care in one visit, including treatment, prescriptions, and delivery.









on your schedule
Skip the unnecessary waiting room,
see a board-certified clinician now.
Prescriptions as needed
Renew or get a new Rx.
On-demand virtual visits
See a physician 24/7.
24/7 care support
We are here to help you.
Download the DrHouse app.
Set up your free account in a minute.
Start a visit with an online doctor. Wait time is less than 15 minutes.
Get an Rx from your preferred pharmacy. Pick up a Rx nearby or get it delivered to you.

on your schedule
Skip the unnecessary waiting room, see a board-certified physician now.
Available in 50 states. Insurance accepted.