|
Read time: 14 min
|
Posted on:
Every practice knows the feeling. A patient calls at 7 p.m. with a fever that will not break, or a question about a medication they just started, and the office is already closed.
Whoever picks up that call, or whatever picks it up, shapes what the patient does next. They either get reassurance and a path forward, or they hang up and decide for themselves, often by driving to urgent care or the emergency room.
Virtual medical answering services exist to handle that moment. But the category has changed a great deal, and the differences between options now have real consequences for patient safety, satisfaction, and practice revenue.
This guide explains what a virtual medical answering service actually is, how it works, the main types available today, what they do well, where they fall short, and why a growing number of practices are rethinking the model entirely.
A virtual medical answering service is a remote service that answers and manages incoming patient calls on behalf of a medical practice, typically when the office is closed, overwhelmed, or short-staffed.
Instead of routing callers to voicemail, the service connects them to a live person, an automated assistant, or in newer models, a clinician, and then relays the relevant information back to the practice.
The word “virtual” simply means the people or systems handling the calls are not sitting at your front desk. They work remotely, use your practice’s protocols, and operate under HIPAA-compliant standards to protect patient information.
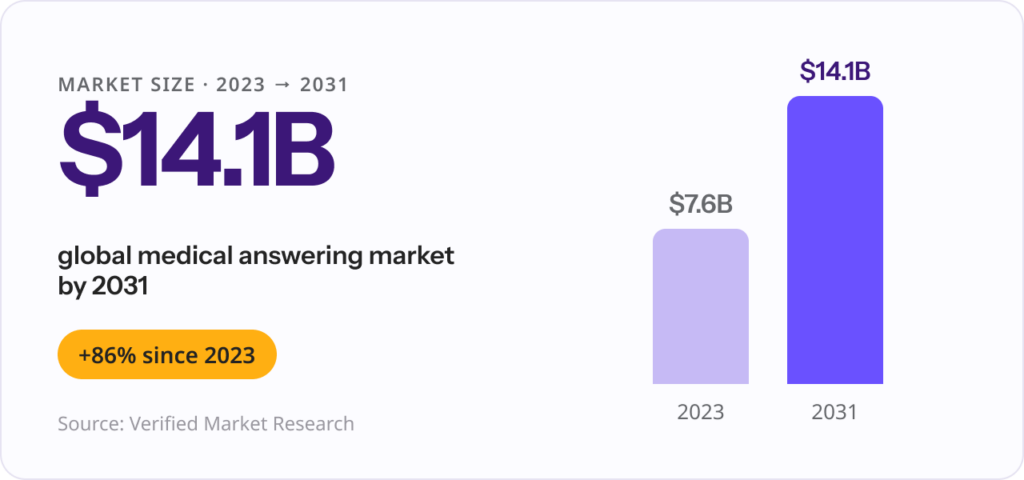
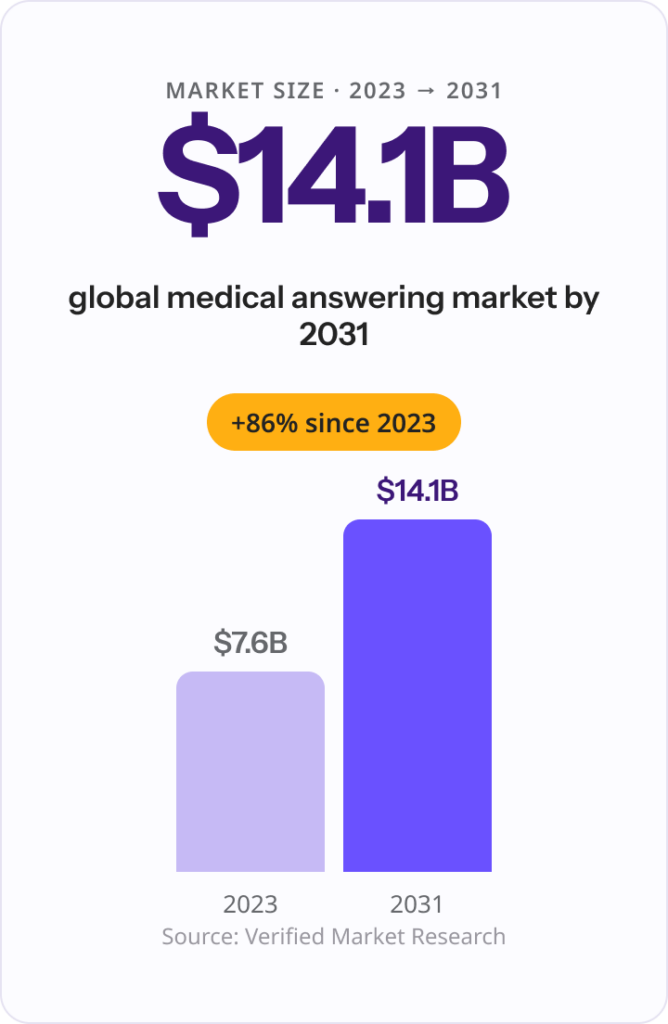
The global medical answering services market reflects how mainstream this has become: it was valued at roughly $7.6 billion in 2023 and is projected to reach about $14.1 billion by 2031, according to Verified Market Research.
What separates a good service from a forgettable one is less about whether the phone gets answered and more about what happens next.
As DrHouse Co-Founder and CEO Ergo Sooru frames it, making sure no call goes to voicemail was always just the starting point, because “a message sitting in an inbox is not the same as a patient who actually got care.” That distinction is the thread that runs through every type of service below.
The exact scope depends on the provider and the plan, but most virtual medical answering services offer some combination of:
The more advanced the service, the further it moves beyond simply taking a message toward actually resolving why the patient called.
The mechanics are designed to be invisible to the patient. They call the number they already know, and everything that follows happens behind the scenes.
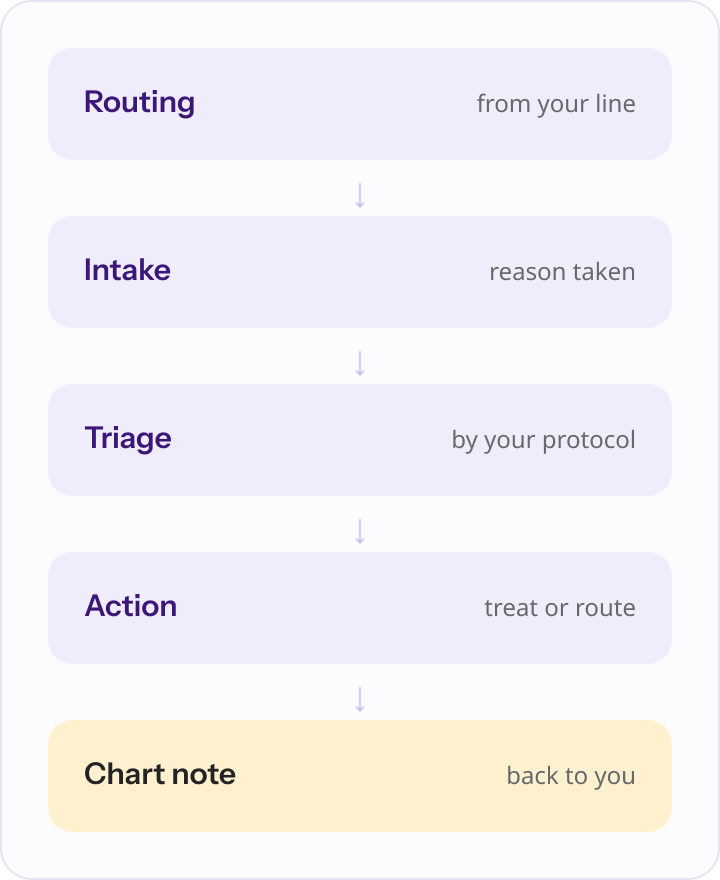
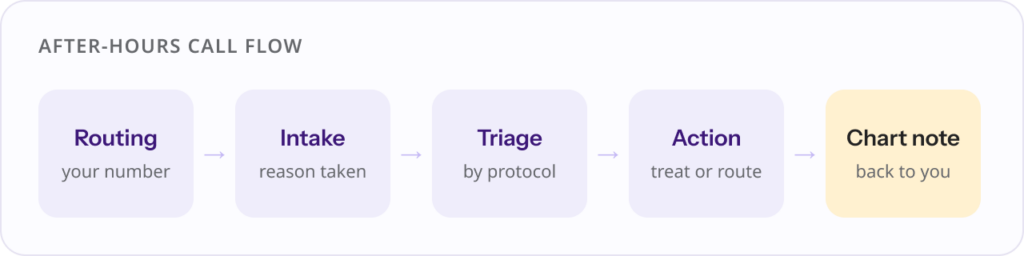
Step by step, a typical after-hours call moves like this:
| Step | What happens | Typically handled by |
|---|---|---|
| 1. Call routing | After-hours and overflow calls forward from your line | Your phone system |
| 2. Greeting and intake | Caller is greeted, basic details and reason collected | Live agent or AI intake |
| 3. Triage | Reason for call assessed against your protocols | Agent, nurse, or AI |
| 4. Action | Message, scheduling, escalation, or direct treatment | Varies by service model |
| 5. Documentation | Summary or chart note sent back to the practice | Service to practice |
The single biggest variable in this flow is step 4. What the service is actually able to do for the patient is what separates one model from another.
Not all services do the same job. They fall into three broad categories, each with a different level of clinical capability.
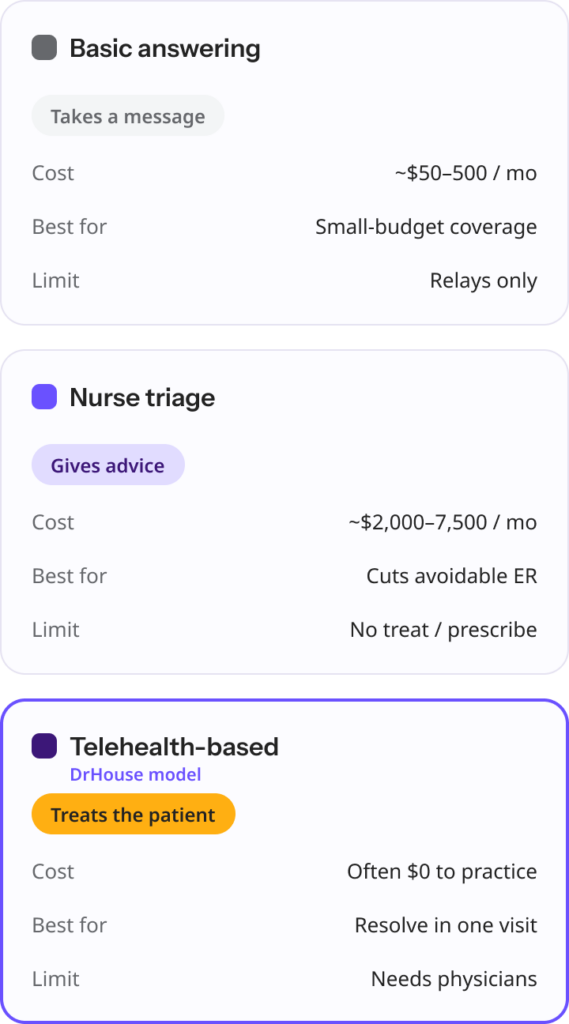
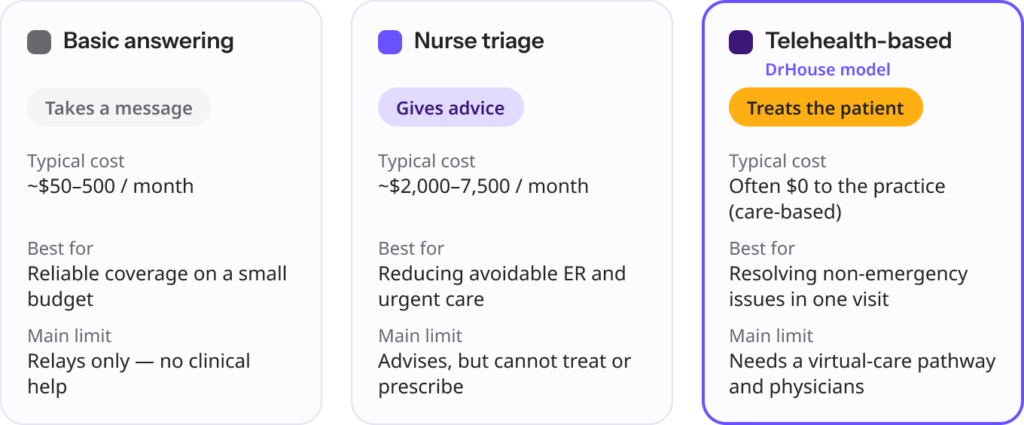
These are the traditional model: trained operators (or an automated system) answer the phone, take a message, and follow simple escalation rules for urgent calls.
They are the most affordable option and work well for practices that only need reliable message capture and call routing. What they do not do is offer clinical guidance. They relay information, they do not resolve it.
A step up in clinical capability, nurse triage lines put a registered nurse on the call. Nurses assess symptoms using evidence-based decision tools, most commonly the Schmitt-Thompson protocols that are considered the gold standard and cover roughly 400 adult and 350 pediatric topics.
The nurse advises the patient on the right level of care: treat at home, see the doctor tomorrow, go to urgent care, or seek emergency help. This model is genuinely effective at preventing unnecessary emergency visits.
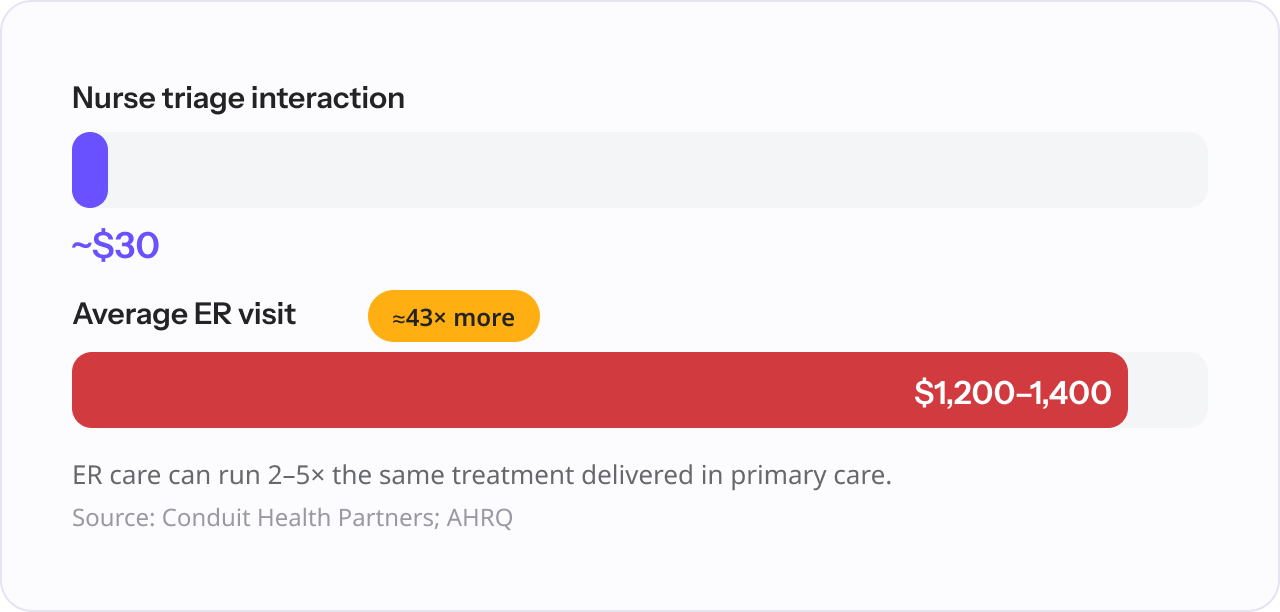
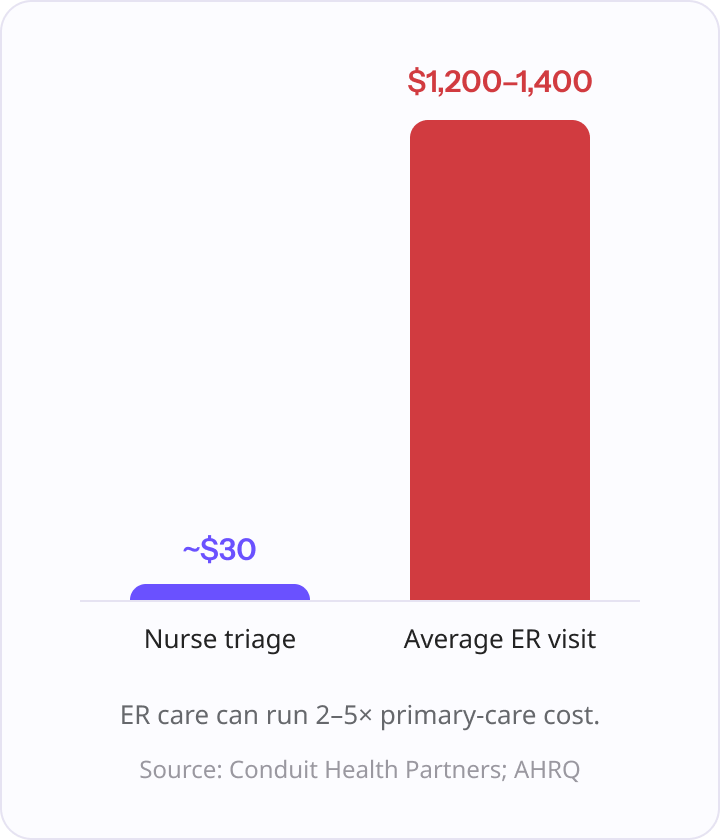
One triage provider, Conduit Health Partners, reports an average nurse-triage interaction costing around $30 against an average emergency department visit of $1,200 to $1,400. The limitation is that nurses advise and direct, but they cannot diagnose or prescribe.
The newest model connects the patient not to a message-taker or an advisor, but to a physician. Using AI-assisted intake to gather information and triage the call, eligible patients are connected to a licensed physician for a video visit.
The physician can evaluate symptoms, diagnose common conditions, and send a prescription to the pharmacy when clinically appropriate. Instead of telling the patient who to call next, the service often resolves the problem in a single interaction.
This is the model DrHouse is built around, and it changes the economics as well as the experience, since care-based services can be offered at no cost to the practice.
| Type | What it does | Best for | Typical cost | Main limitation |
|---|---|---|---|---|
| Basic answering | Takes messages, screens and routes urgent calls | Reliable coverage on a small budget | Roughly $50 to $500 per month | No clinical help; relays only |
| Nurse triage | RNs assess symptoms and advise on the right level of care | Reducing unnecessary ER and urgent care visits | Roughly $2,000 to $7,500 per month, or per-minute | Advises and directs, cannot treat or prescribe |
| Telehealth-based | Physicians evaluate, diagnose, and treat via video | Resolving non-emergency issues in one interaction | Often $0 to the practice (care-based model) | Requires a virtual-care pathway and physician network |
Costs vary widely because providers bill differently. Some charge per call, some per minute, and some by monthly subscription, so two practices with the same provider can pay very different amounts depending on call volume and complexity.
Even the most basic service solves a real and measurable problem: it keeps the practice reachable. That matters more than it might sound.
The average practice fields a lot of calls. In a recent MGMA survey of more than 300 practice leaders, 59 percent reported handling 30 or more calls a day, and 36 percent said at least 11 percent of their calls go unanswered or roll to voicemail during peak times.

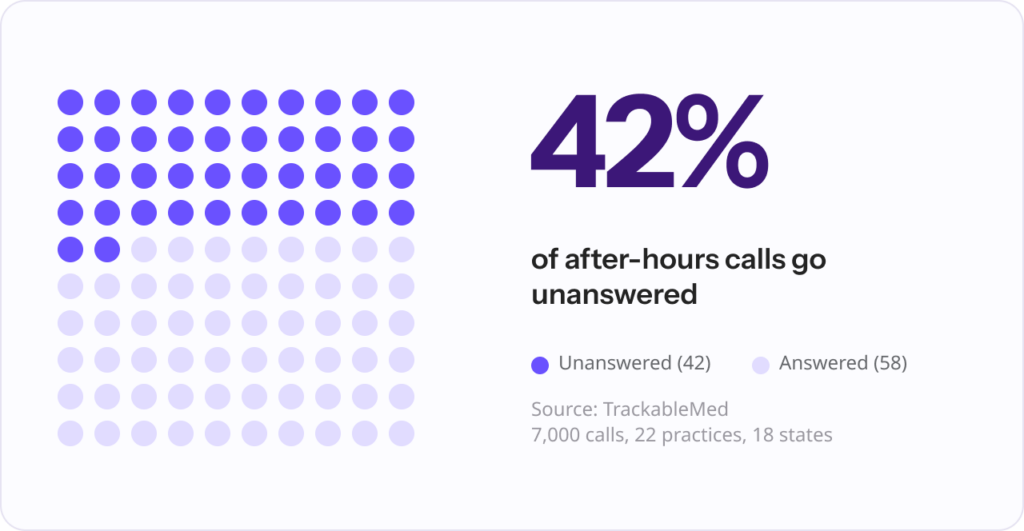
The after-hours picture is worse. An analysis by TrackableMed of 7,000 calls across 22 practices in 18 states found that practices missed about 42 percent of incoming calls. When patients reach voicemail, many simply hang up, and a patient with an urgent concern who cannot get through will often call another provider instead.
A good answering service addresses this directly. The strongest benefits include:
The traditional model has a structural ceiling. It can make sure a call is answered, but for most services, answering is where the help ends. The patient still has an unresolved medical concern, and now they are waiting for a callback that may not come until morning.
This gap has a price, and it shows up in two places: the patient’s care and the practice’s books.
| The gap | What the data shows |
|---|---|
| Missed calls | Practices missed roughly 42% of incoming calls in an analysis of 7,000 calls across 22 practices in 18 states. (Source: TrackableMed) |
| Unanswered at peak | 36% of practice leaders report 11%+ of calls going unanswered or to voicemail at busy times. (Source: MGMA survey) |
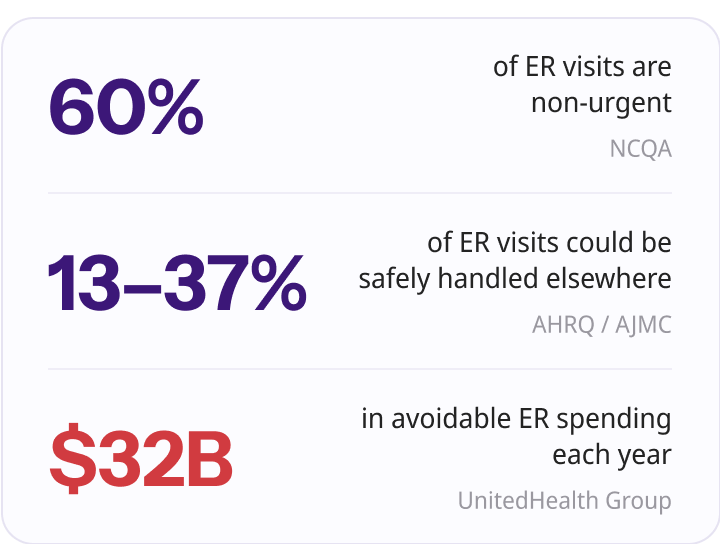
| After-hours demand | About one in four after-hours primary care calls are for medically non-urgent issues. (Source: BMC Family Practice (peer-reviewed)) |
| Avoidable ER use | Up to two-thirds of privately insured ER visits are considered avoidable, adding an estimated $32 billion a year. (Source: UnitedHealth Group, via US News) |
| Care setting cost | ER care can cost two to five times the same treatment delivered in primary care. (Source: AHRQ) |
A message taken at midnight does not lower a fever, refill a lapsed prescription, or rule out something serious. So the patient self-triages. Sometimes that means waiting and getting worse, and sometimes it means an expensive trip to the ER for something a physician could have handled in ten minutes by video.
Sooru describes this as the structural limit of the old model: a traditional service can tell a worried patient that someone will call them back, but “it cannot examine them, reassure them, or treat them,” and that gap is where patients give up and drive to the emergency room.
Either way, the practice loses visibility, and the patient relationship takes a quiet hit.
Two technologies have matured enough to close the gap: AI-assisted intake and physician-led telehealth. Together, they turn the after-hours call from a relay into actual care.
AI handles the front of the call, greeting the patient, gathering structured information, and triaging against the practice’s rules quickly and consistently.
Telehealth handles the back of it, connecting eligible patients to a licensed physician for a video visit within minutes.
The physician evaluates, diagnoses, and treats common conditions, sending prescriptions to the pharmacy when appropriate. The practice receives a chart note instead of a message, and the patient gets resolution instead of a callback.
Sooru sees this as the technology finally catching up to what patients always wanted: answer the phone, understand why someone is calling, and connect them with a real physician in minutes, “all without the practice lifting a finger.” In his words, “the house call is back, just rebuilt for how people actually live now.”
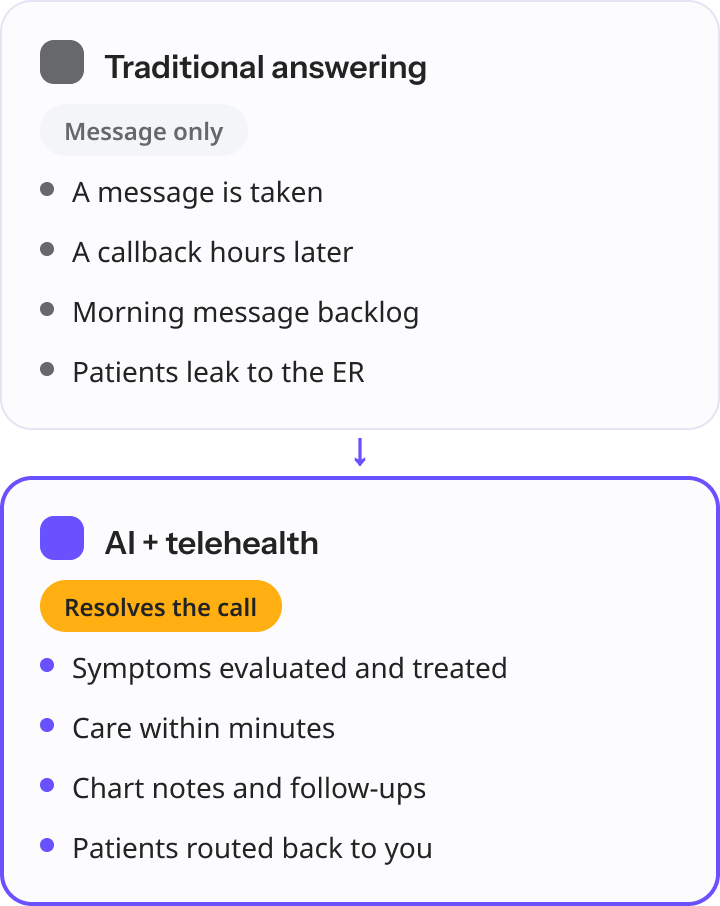
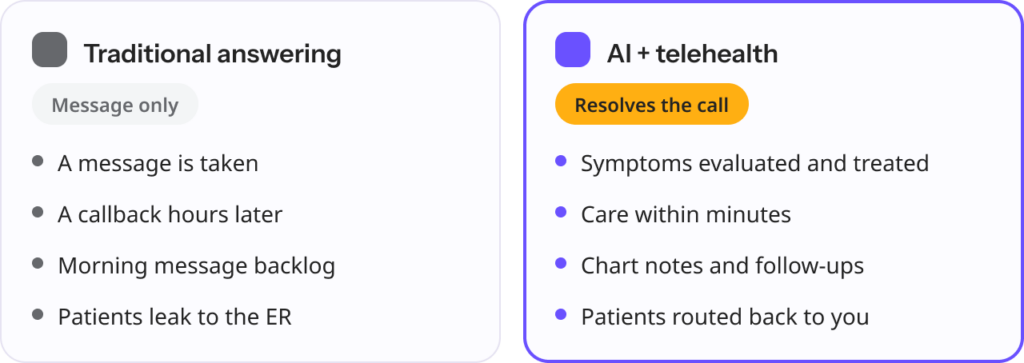
| Traditional answering service | Modern AI and telehealth model | |
|---|---|---|
| What the caller receives | A message is taken | Symptoms are evaluated and often treated |
| Speed to help | A callback hours later | Care within minutes |
| After-hours outcome | “Someone will call you back” | Diagnosis, prescription, and documentation |
| Next-day practice workload | A backlog of messages to clear | Chart notes and clearly defined follow-ups |
| Cost model | Per call, per minute, or subscription | Often care-based, with no fee to the practice |
| Patient leakage | High, often to the ER or urgent care | Reduced, with care routed back to you |
A common worry is that adding a service means new software, new logins, and staff retraining. With the better modern options, it does not.
The cleanest implementations work with the phone system you already have. Calls forward from your existing number, so patients do not need to learn anything new.
There is no software to install and no platform for your staff to manage. Setup is usually a matter of confirming when calls should route to the service and what types of requests it should handle, which many practices can do quickly.
Just as important is what comes back. After each interaction, documentation returns to your practice, commonly by fax in current workflows, so notes can be added to the patient record as part of your normal morning routine. You do not need a direct EHR integration project to get full visibility into what happened after hours.
The result is a service that sits alongside your operations rather than inside them. Your team starts the day with clear documentation and defined follow-ups instead of a voicemail backlog and a wave of callbacks.
The shift is less about disliking answering services and more about a change in what practices expect after-hours coverage to accomplish. Paying every month to take messages starts to feel like paying for half a solution once a better one exists.
Three pressures are driving the move. First, patient expectations have caught up with every other on-demand service in their lives, and a callback tomorrow no longer feels acceptable for a concern that feels urgent tonight.
Second, the financial math is hard to ignore once a practice sees the revenue tied up in missed and unresolved calls. Third, continuity of care has become a competitive issue: when a patient’s after-hours problem gets solved by an outside service that keeps them attributed to the practice and routes follow-ups back, the practice protects the relationship instead of risking it.
Telehealth-based coverage answers all three at once, and often at no cost to the practice, because revenue is generated from completed patient visits rather than monthly fees. That is a meaningfully different proposition from the per-call or per-minute pricing of legacy services.
The shift in mindset, as Sooru puts it, is that practices are realizing they were paying to take messages, not to solve problems. When the after-hours call ends with the patient treated and a chart note waiting in the morning, “you are no longer managing a backlog, you are extending your care.”
A virtual medical answering service makes sure patient calls are handled when your office cannot handle them.
That is valuable on its own, given how many calls go unanswered and how quickly patients move on when they cannot reach you. But the category is no longer one thing. Basic services take messages, nurse triage lines advise, and telehealth-based services actually treat.
The right choice depends on what you want the after-hours call to accomplish. If the goal is simply to capture messages reliably, a traditional service does that.
If the goal is to genuinely resolve patient concerns, reduce avoidable ER visits, protect the patient relationship, and start each morning with documentation instead of a backlog, the model worth looking at is physician-led telehealth coverage that connects to your existing workflow and keeps every patient attributed to you.
DrHouse provides exactly that: AI-assisted intake, licensed physicians treating eligible patients by video, prescriptions sent to the pharmacy when appropriate, and chart notes returned to your practice, all at no cost to your office. It is after-hours coverage built as an extension of your care, not a replacement for it.
Content on the DrHouse website is written by our medical content team and reviewed by qualified MDs, PhDs, NPs, and PharmDs. We follow strict content creation guidelines to ensure accurate medical information. However, this content is for informational purposes only and not a substitute for professional medical advice, diagnosis, or treatment. For more information read our medical disclaimer.
Always consult with your physician or other qualified health providers about medical concerns. Never disregard professional medical advice or delay seeking it based on what you read on this website.
If you are experiencing high fever (>103F/39.4C), shortness of breath, difficulty breathing, chest pain, heart palpitations, abnormal bruising, abnormal bleeding, extreme fatigue, dizziness, new weakness or paralysis, difficulty with speech, confusion, extreme pain in any body part, or inability to remain hydrated or keep down fluids or feel you may have any other life-threatening condition, please go to the emergency department or call 911 immediately.
Experience 24/7 complete care in one visit, including treatment, prescriptions, and delivery.









on your schedule
Skip the unnecessary waiting room,
see a board-certified clinician now.
Prescriptions as needed
Renew or get a new Rx.
On-demand virtual visits
See a physician 24/7.
24/7 care support
We are here to help you.
Download the DrHouse app.
Set up your free account in a minute.
Start a visit with an online doctor. Wait time is less than 15 minutes.
Get an Rx from your preferred pharmacy. Pick up a Rx nearby or get it delivered to you.

on your schedule
Skip the unnecessary waiting room, see a board-certified physician now.
Available in 50 states. Insurance accepted.