|
Read time: 15 min
|
Posted on:
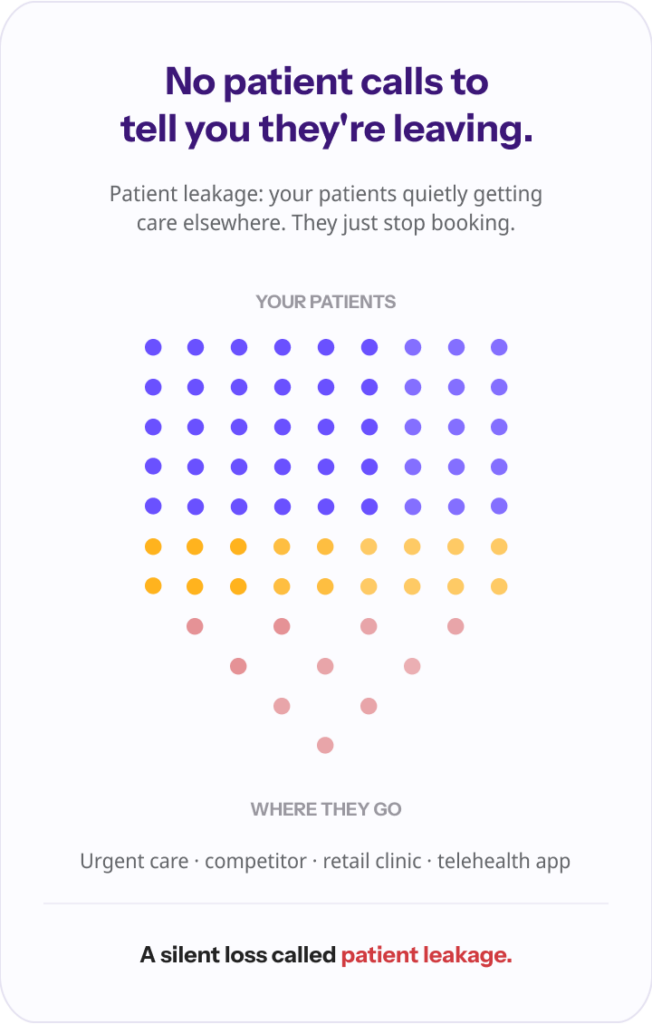
No patient ever calls to tell you they are leaving. That is the whole problem in one sentence. A patient does not send a breakup note. They just stop booking.
Maybe they went to the urgent care near their office for a sinus infection because they couldn’t get in to see you that week, had a fine visit, and quietly decided that was easier. Maybe they called on a Saturday, reached your voicemail, and found someone who picked up.
You don’t get an alert when it happens. You find out months later, if you find out at all, when the schedule looks a little thinner, and you can’t quite say why.
That slow, silent loss has a name: patient leakage. And for most practices, it is bigger, quieter, and more fixable than they realize. This article is about seeing it clearly, what it is, where it comes from, and what it actually costs.
Patient leakage is the movement of your patients outside your practice or network for care you could have provided. The patient is nominally yours. The visit, the revenue, and a little piece of the relationship all go to someone else.
The opposite of leakage is sometimes called keepage, the share of care your patients actually receive from you. Every practice sits somewhere on that spectrum, whether or not anyone is measuring it.
Your leakage rate is simply the percentage of your patients’ care that happens elsewhere, and under value-based and attribution-based models, where you are accountable for a population’s cost and outcomes, that number stops being a marketing curiosity and starts being a financial one.
When a patient you are responsible for gets a duplicate test at an outside imaging center, you can inherit the cost, the gap in the record, and the worse-coordinated outcome all at once.
Here is the part most coverage of this topic gets wrong, though.
“When people say ‘patient leakage,’ they almost always mean referrals, a specialist sending business out the door. For a primary care practice, that is not where most patients are lost. They are lost on a Tuesday night and a Saturday afternoon, when someone needed care, couldn’t reach you, and found someone who was open.” Ergo Sooru, Co-Founder & CEO, DrHouse.
That distinction matters enough to break the problem into its real parts.
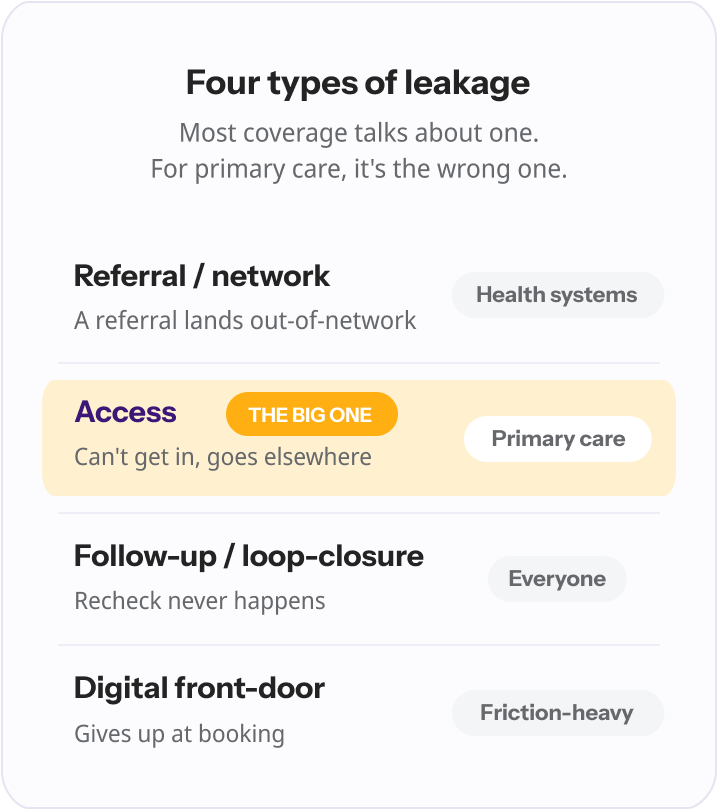
Leakage is not one thing. It leaks from different seams, and the seam that gets all the attention is rarely the one bleeding the most in a primary care practice.
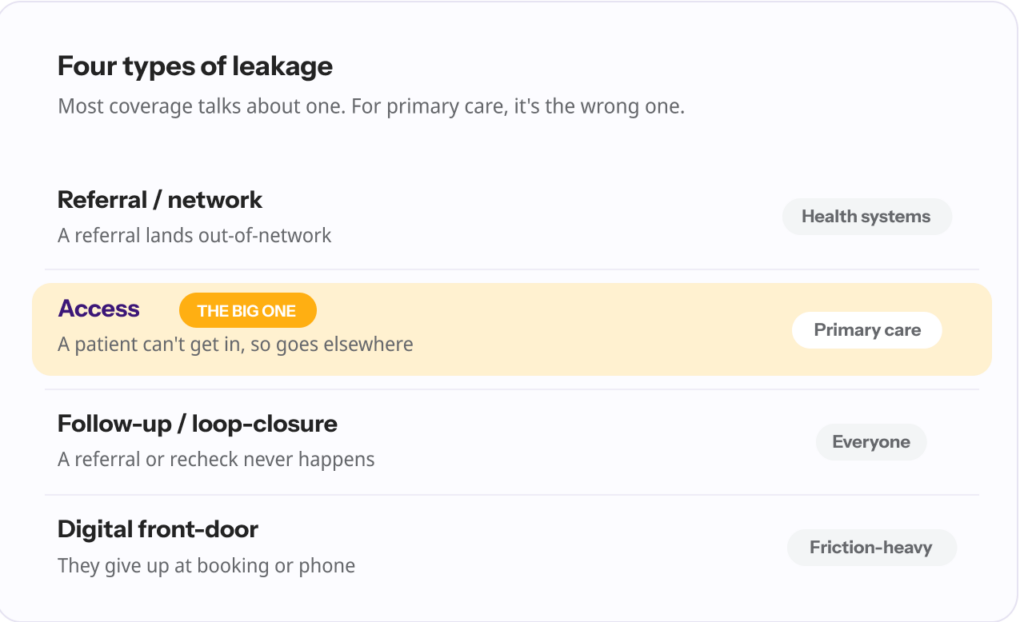
| Type of leakage | What it is | A typical example | Who it hits hardest |
|---|---|---|---|
| Referral / network leakage | A patient you refer ends up with an out-of-network specialist or imaging center | You refer for an MRI; the patient books at an unaffiliated imaging center | Health systems, specialty groups |
| Access leakage | A patient can’t get in when they need to, so they go elsewhere | Can’t get a same-day slot; goes to urgent care instead | Primary care, independent practices |
| Follow-up / loop-closure leakage | A referral or follow-up is recommended but never actually happens with you | A specialist referral is written, never scheduled, never tracked | Everyone; especially busy practices |
| Digital front-door leakage | The patient gives up at the booking, phone, or portal stage | Can’t book online at 10 p.m., books with a telehealth app instead | Practices with friction-heavy access |
The reason this taxonomy matters is that you cannot fix a leak you have misdiagnosed. If you assume leakage is a referral problem and buy a referral-tracking tool, but your real loss is patients who can’t reach you after hours, you have spent money solving the wrong thing.
Strip away the jargon and patient leakage comes down to a handful of very human reasons. They are worth naming plainly, because each one points at something you can actually change.
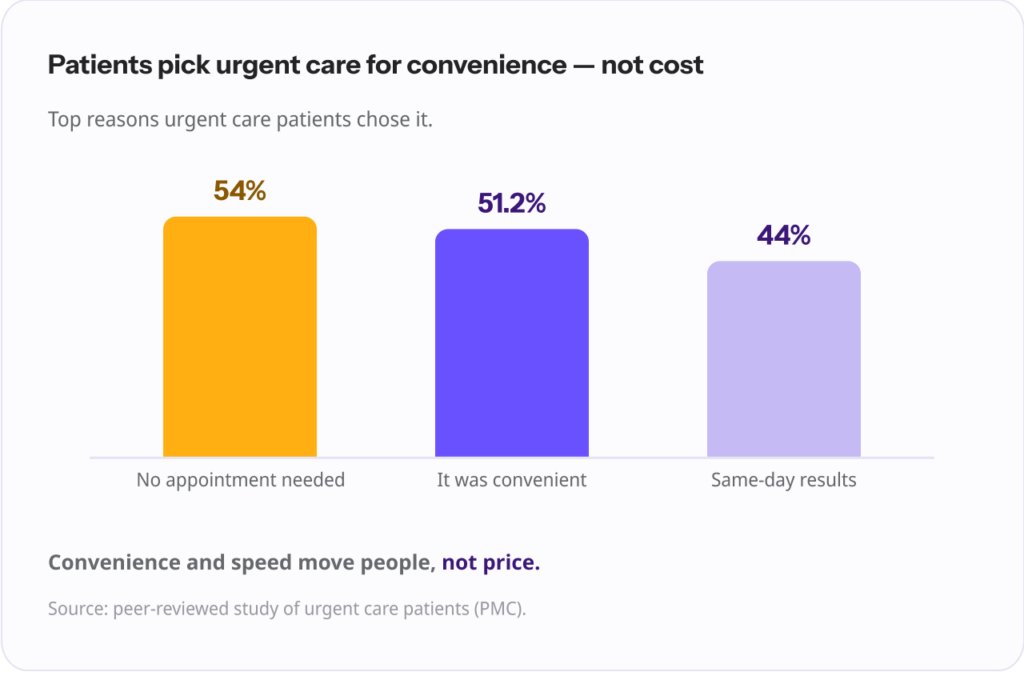
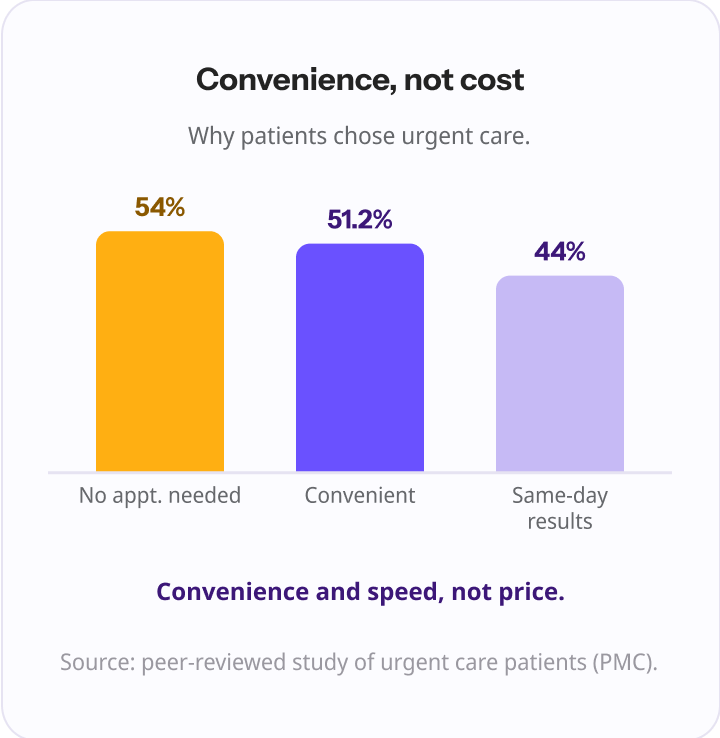
This is the big one, and the data on where patients go instead is unambiguous. When people choose an urgent care over their own doctor, it is not mainly about money.
In one study of urgent care patients, 54% chose it because they didn’t have to make an appointment, 51.2% because it was convenient, and roughly 44% because they could get same-day results. Convenience and speed, not cost, are what move people.
And the alternatives have multiplied. The number of urgent care centers in the U.S. grew from about 6,100 in 2013 to more than 9,000 by 2022. Retail and convenient-care clinics have expanded alongside them, to the point that they are now reshaping a roughly $300 billion primary care market, with a majority of patients saying they intend to keep using retail clinics.
Every one of those locations is a door that opens faster than a next-week appointment. When your access tightens, theirs is right there.
Illness does not keep office hours. A fever spikes at 8 p.m., a child’s ear starts hurting on Sunday, a UTI flares on a holiday weekend.
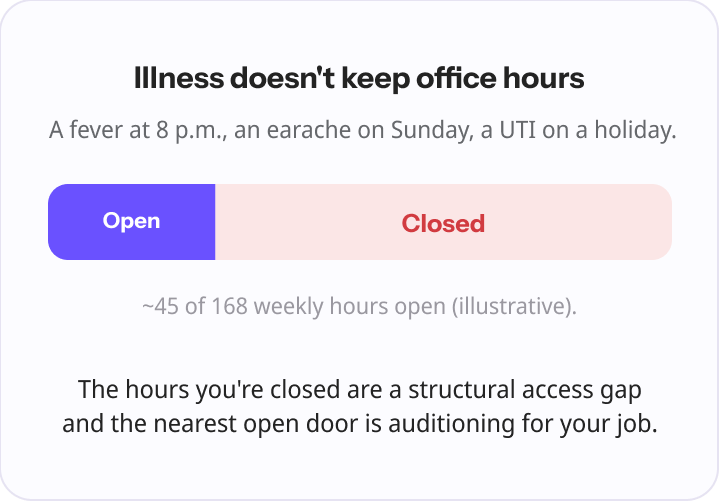
If the patient cannot reach you in those moments, they are not going to wait politely until Monday. They are going to find care, and the place they find is auditioning for your job.
“Every after-hours call that hits a voicemail is a patient auditioning your competitor. They go to the urgent care down the road, they have a perfectly fine experience, and the next time they don’t even call you first. You didn’t lose one visit, you lost the relationship, and you never saw it happen.” Ergo Sooru, Co-Founder & CEO, DrHouse.
After-hours and weekends are a structural access gap for most practices, and structural is the key word. It is not a staffing failure or a one-off. It is simply that the practice is closed, predictably, for a large share of the hours patients get sick. That predictability is also what makes it addressable, but more on that in the companion piece.
When you do refer, the patient does not always land where you intended. Specialist availability, wait times, reputation, plain convenience, and weak follow-up all pull patients out of network.
And once a patient is sitting in another system’s waiting room, that system has every incentive to keep them.
Then there is the slow drip: long waits, phone tag, a booking process that takes three calls, a portal nobody can log into, a no-show that never gets rescheduled. None of these is dramatic.
Together they teach patients that getting care from you is work, and that the app or the clinic down the street is less work. Friction is leakage in slow motion.
Here is where it gets uncomfortable, and where the numbers deserve a careful eye, because this is a topic where confident-sounding statistics get copied around the internet without anyone checking the original source. So a note on sourcing: the figures below range from solid survey data to widely repeated industry estimates, and they are labeled accordingly.
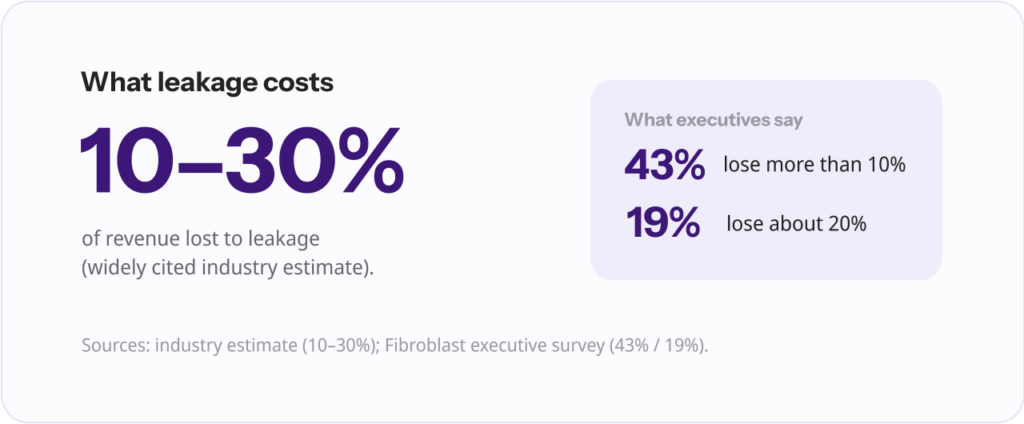
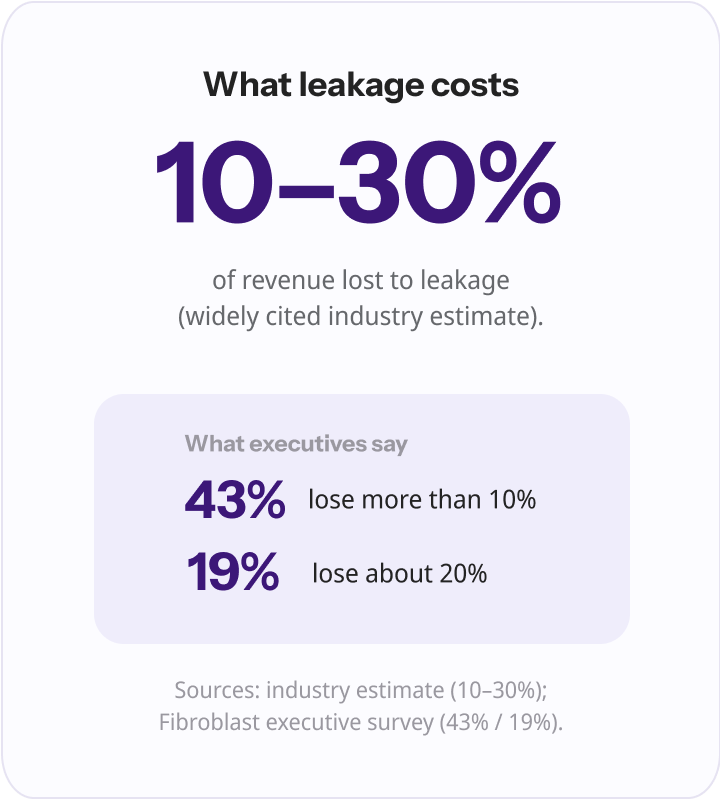
The most commonly cited range is that health systems lose somewhere between 10% and 30% of revenue to patient and referral leakage. Treat that as a directional industry estimate rather than a precise measurement; it appears across many vendor and trade sources without a single clean origin.
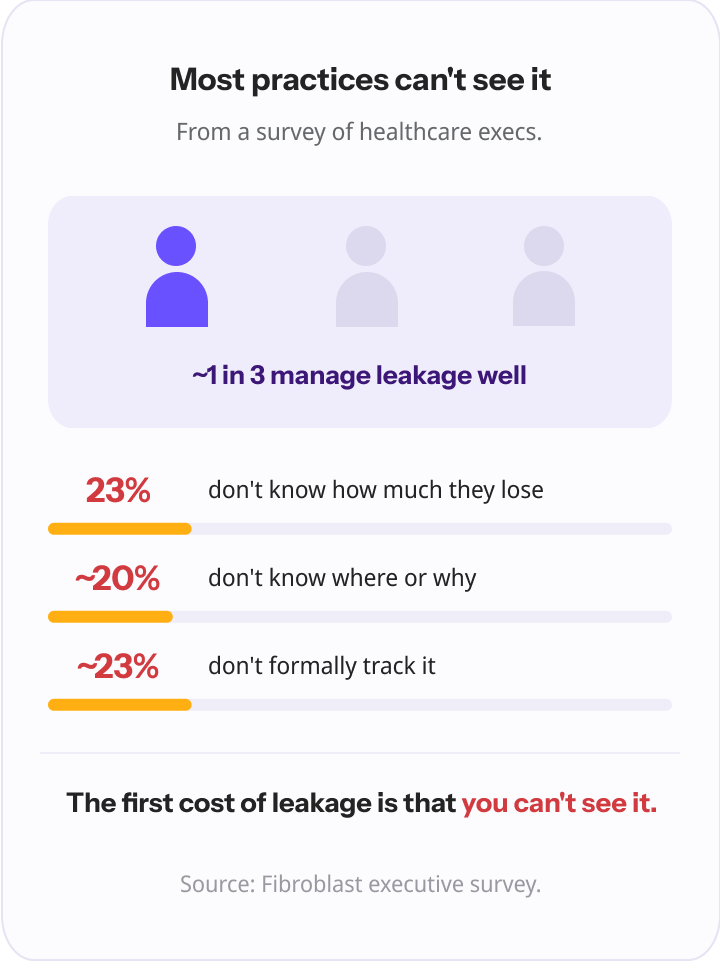
The sturdiest data point comes from a survey of healthcare executives. In it, 43% said their organization loses more than 10% of revenue to patients going elsewhere, and 19% put the figure at 20%.
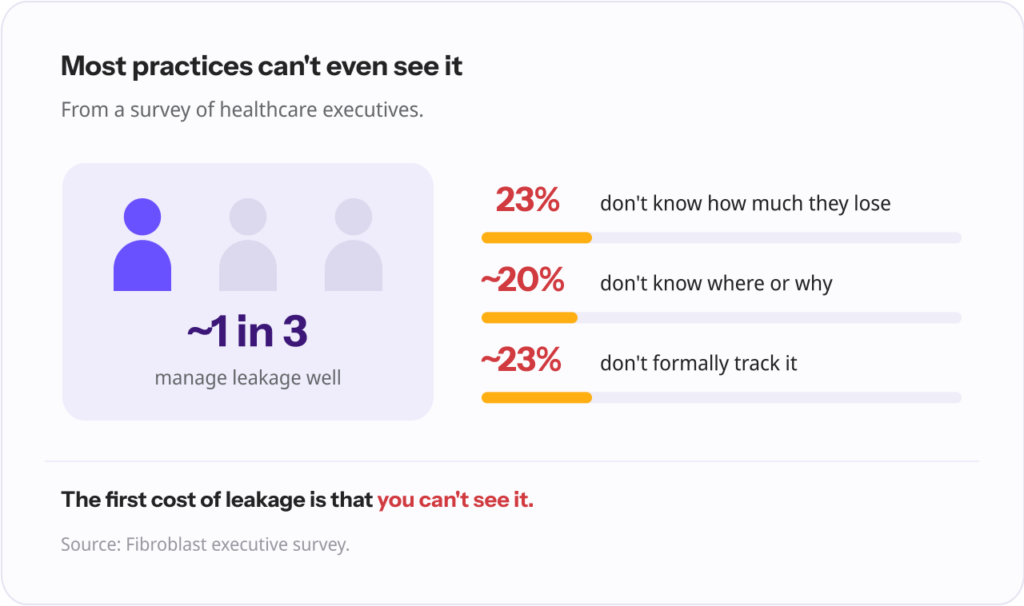
The more revealing finding sits next to those: 23% of leaders said they did not know how much they were losing, and about 20% said they did not understand where or why leakage was happening at all. Roughly a quarter were not formally tracking it, and only about one in three felt they managed it well. The first cost of leakage, in other words, is that most organizations cannot see it.
You will also see eye-catching per-provider numbers, that leakage costs somewhere between $821,000 and $971,000 per physician per year, or that 55% to 65% of referrals go out of network, and a national figure of around $150 billion a year.
These are worth knowing, but they trace back to vendor estimates and older analyses with murky provenance, so hold them loosely.
The honest takeaway is not a precise dollar figure. It is that the loss is large, it compounds, and most practices are flying blind on it.
| Figure | What it represents | Source and tier |
|---|---|---|
| 10% to 30% of revenue | Estimated share lost to patient/referral leakage | Widely cited industry estimate |
| 43% lose >10%; 19% lose ~20% | Executives’ own estimate of revenue lost | Fibroblast executive survey (trade press) |
| ~23% don’t know / ~23% don’t track | Leaders who can’t quantify their leakage | Fibroblast executive survey (trade press) |
| $821K to $971K per physician/yr | Estimated annual loss per physician | Vendor estimate, older, hold loosely |
| ~$150 billion/yr | Estimated U.S. national cost | Industry estimate, fuzzy attribution |
And the dollars are only the visible part. Every leaked visit is also a hole in the record. The outside urgent care does not send you a tidy note by default.
Results get repeated because nobody had the prior ones, histories get fragmented, and the continuity that makes primary care actually work, the thing that lets you catch the pattern across visits, frays a little with each episode of care that happens somewhere you never hear about.
Because leakage is silent, you have to go looking for it. The good news is that you do not need an enterprise analytics platform to start. You need to pay attention to a few signals you already have.
| Warning sign | What it is telling you | Where to look |
|---|---|---|
| Rising after-hours voicemail volume | Patients are reaching for you when you’re closed, and not all of them wait | Phone system / answering service logs |
| Patients mention outside urgent care or ER visits | Care is happening without you, and without a note | Visit notes, intake conversations |
| Low same-day appointment fill rate | Access is too tight; patients are being turned toward alternatives | Scheduling data |
| No-shows and abandoned bookings creeping up | Friction or competition is pulling patients away | Schedule, online booking analytics |
| Referrals you can’t confirm were completed | Loops are open; follow-up care may be leaking | Referral tracking, specialist feedback |
If you can estimate your leakage rate at all, even roughly, you are ahead of the roughly one in four organizations that don’t track it.
The point of this exercise is not precision. It is to turn an invisible problem into a visible one, because the moment you can see where patients are leaving, the fix usually becomes obvious.
“The thing that makes leakage so dangerous is that it’s silent. There’s no alert when a patient quietly starts going somewhere else. By the time it shows up in your numbers, you’ve been losing people for months. You can’t fix what you can’t see, and most practices simply can’t see it yet.” Ergo Sooru, Co-Founder & CEO, DrHouse.
That is the right question, and it deserves a real answer, which is why it gets its own article. The short version: most leakage in a primary care practice is access leakage, and access is the part you have the most control over.
The fixes fall into a few buckets: closing same-day access gaps, covering the hours you are closed, tightening referrals so loops actually close, and stripping out the everyday friction that teaches patients to go elsewhere.
Of those, the highest-return move for most practices is the most structural one: making sure that when a patient needs care after hours, they can reach a clinician and come back to you, rather than disappearing into the nearest open door. That is the gap that quietly feeds urgent care, and it is very fixable.
Physician-led after-hours coverage is one way practices close it without adding staff, and we walk through the full playbook, including how to think about same-day access and referral loops, in the companion piece on reducing patient leakage.
Patient leakage is usually framed as a referral-tracking problem for hospitals. For the practice owner, the family physician, the manager watching the schedule, it is something more personal and more fixable: it is patients leaving because they couldn’t get to you when they needed to.
It is mostly about access, and it is mostly invisible until it has already cost you.
So the first move is not a tool or a vendor. It is to look honestly at where your patients actually go when they can’t reach you, and to recognize that the silence is the problem, not the absence of one.
Once you can see the leaks, you can close them. Start with the hours you are closed.
Patient leakage is when patients receive care outside your practice or network, for example at an urgent care, a competitor, a retail clinic, or a telehealth app, when you could have provided that care. It reduces revenue and fragments the patient’s record and continuity of care.
Referral leakage is one type of patient leakage: it happens when a referred patient ends up with an out-of-network specialist or facility. Patient leakage is the broader category, which also includes access leakage (patients who can’t get in and go elsewhere), follow-up leakage, and digital front-door leakage.
Industry estimates commonly put the loss at 10% to 30% of revenue, and in one survey of healthcare executives, 43% said they lose more than 10% of revenue to patients going elsewhere. Many leaders, however, cannot quantify their own number, and a sizable share do not formally track it at all.
The leading causes are access related: patients who can’t get a timely or same-day appointment, and practices being closed after hours and on weekends. Out-of-network referrals, open referral loops, and everyday friction (long waits, phone tag, clunky booking) add to it. Patients overwhelmingly leave for convenience and speed, not price.
Look for warning signs you already have access to: rising after-hours voicemail volume, patients mentioning outside urgent care or ER visits, a low same-day fill rate, climbing no-shows, and referrals you can’t confirm were completed. Most practices are not tracking this yet, so simply starting to look puts you ahead.
Content on the DrHouse website is written by our medical content team and reviewed by qualified MDs, PhDs, NPs, and PharmDs. We follow strict content creation guidelines to ensure accurate medical information. However, this content is for informational purposes only and not a substitute for professional medical advice, diagnosis, or treatment. For more information read our medical disclaimer.
Always consult with your physician or other qualified health providers about medical concerns. Never disregard professional medical advice or delay seeking it based on what you read on this website.
If you are experiencing high fever (>103F/39.4C), shortness of breath, difficulty breathing, chest pain, heart palpitations, abnormal bruising, abnormal bleeding, extreme fatigue, dizziness, new weakness or paralysis, difficulty with speech, confusion, extreme pain in any body part, or inability to remain hydrated or keep down fluids or feel you may have any other life-threatening condition, please go to the emergency department or call 911 immediately.
Experience 24/7 complete care in one visit, including treatment, prescriptions, and delivery.









on your schedule
Skip the unnecessary waiting room,
see a board-certified clinician now.
Prescriptions as needed
Renew or get a new Rx.
On-demand virtual visits
See a physician 24/7.
24/7 care support
We are here to help you.
Download the DrHouse app.
Set up your free account in a minute.
Start a visit with an online doctor. Wait time is less than 15 minutes.
Get an Rx from your preferred pharmacy. Pick up a Rx nearby or get it delivered to you.

on your schedule
Skip the unnecessary waiting room, see a board-certified physician now.
Available in 50 states. Insurance accepted.