|
Read time: 12 min
|
Posted on:
If your practice has ever started a Monday with a stack of weekend voicemails, you already understand the problem a nurse triage line is meant to solve.
Patients get sick when you are closed. Without somewhere for those calls to go, they wait, they worry, or they leave to find care elsewhere. A nurse triage line gives them a clinician to talk to instead of a recording.
This guide is for the person making the decision: the practice owner, the office manager, the physician who is tired of being paged at midnight.
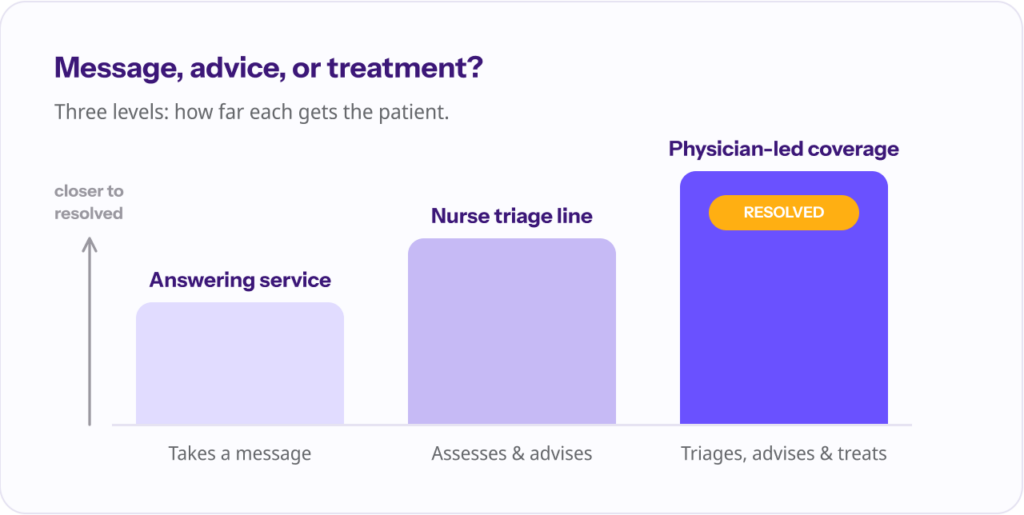
It covers what a nurse triage line actually is, how it works, what it costs, how to choose one, and one question worth asking before you sign anything: do you want your after-hours calls routed, or resolved?
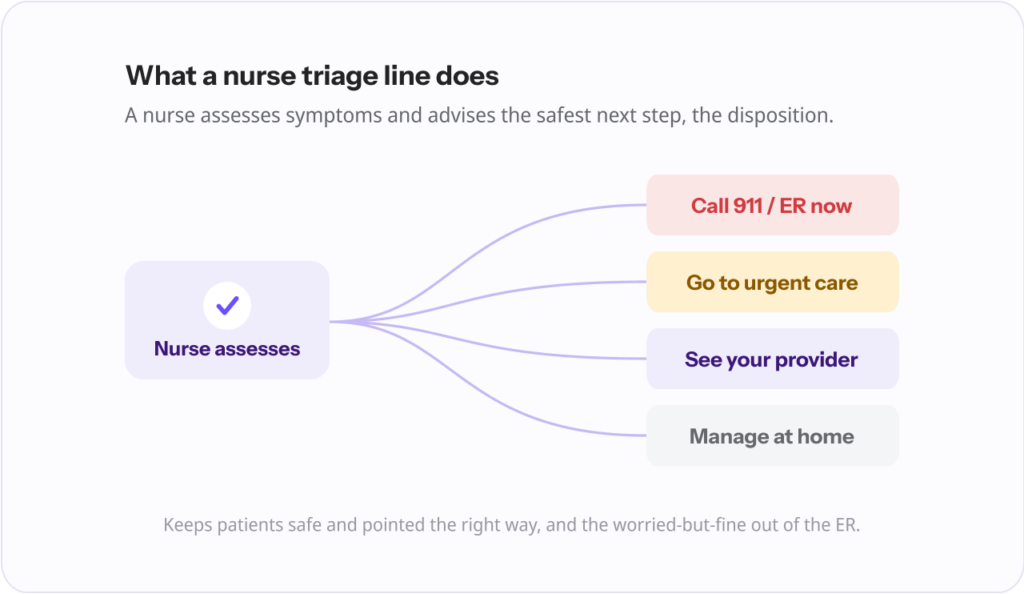
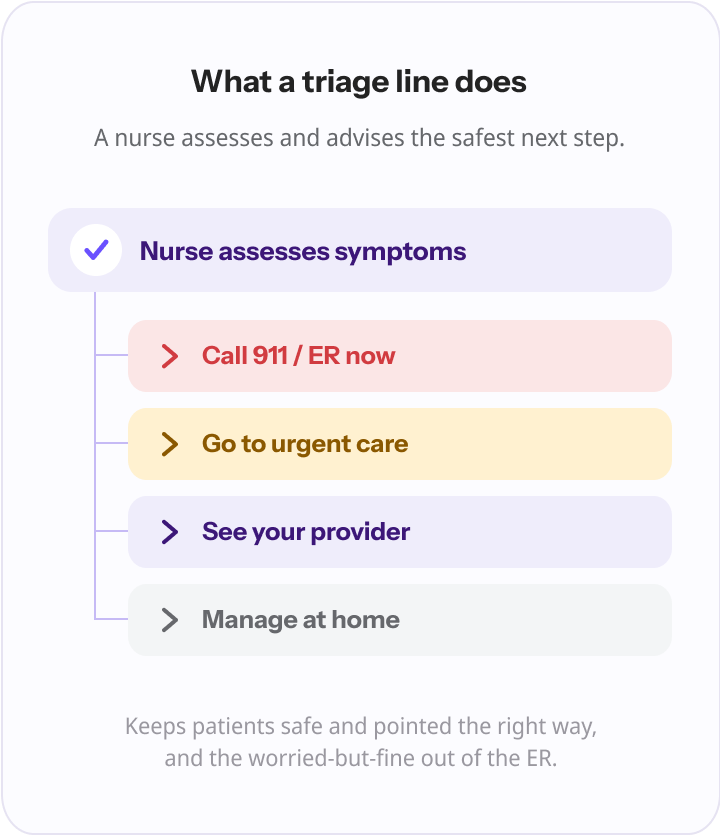
A nurse triage line is a service that answers patients’ calls when they cannot get to your practice, and connects them to a registered nurse who assesses their symptoms and advises on what to do next.
That advice, called a disposition, sorts the patient into the right level of care: call 911 or go to the emergency room now, go to urgent care, schedule with your provider, or manage it safely at home.
From the patient’s side it is simple. They call your usual number, the call routes to the triage line, and a nurse picks up.
From your side, it is a way to make sure that the hours you are closed (nights, weekends, holidays) and the moments you are slammed (overflow during a busy clinic day) do not become dead ends for the people who depend on you.
It is worth being precise about what a nurse triage line is for: it keeps patients safe and pointed in the right direction, and it keeps the worried-but-fine ones out of the emergency room. That is genuinely valuable. It is also, as we will see, where its job ends.
The mechanics are straightforward, and most outsourced services follow the same shape.
| Step | What happens | What your practice gets |
|---|---|---|
| 1. Call routing | After-hours and overflow calls forward from your existing number to the triage line | Patients reach a clinician instead of voicemail |
| 2. Nurse assessment | A registered nurse assesses symptoms using standardized clinical protocols | Consistent, protocol-based decisions, not ad hoc judgment |
| 3. Disposition | The nurse advises the safest next step: ER, urgent care, see your provider, or home care | Patients directed to the right level of care |
| 4. Documentation | The call and its disposition are documented and sent back to you | A record of after-hours activity, usually by the next business day |
The quality of the whole thing rests on step two. Reputable triage lines run on standardized decision-support protocols, most commonly the Schmitt-Thompson protocols, which a triage vendor describes as covering roughly 350 pediatric and 400 adult topics. Those protocols are what keep a 2 a.m. decision consistent and defensible rather than dependent on whichever nurse happens to pick up.
A good service also has a clear escalation pathway for true emergencies and red-flag symptoms, so the genuinely sick patient is moved quickly rather than talked through home care.
The first real decision is whether to build it or buy it. A few practices run triage in-house, often using nurse triage software to guide their own staff. Most that want around-the-clock coverage outsource it, because staffing a phone line overnight is its own headache.
| Factor | In-house nurse triage | Outsourced nurse triage line |
|---|---|---|
| Upfront cost | Hiring and training nurses, plus triage software | Low; turnkey |
| 24/7 coverage | Hard to staff overnight, weekends, and holidays | Built in |
| Staffing burden | High; your own nurses cover the shifts | None |
| Control | Full | You set the protocols and rules; the vendor executes them |
| Setup time | Weeks to months | Days |
The honest trade-off is control versus burden. In-house keeps everything under your roof but asks your already-stretched nurses to cover the hours nobody wants.
Outsourcing hands off the staffing problem, but means trusting a third party with your patients at their most anxious. For most small and mid-sized practices, the math favors outsourcing the after-hours window, the demand is too thin and too unpredictable to justify staffing it yourself.
Pricing varies by model, and it pays to look past the headline number.
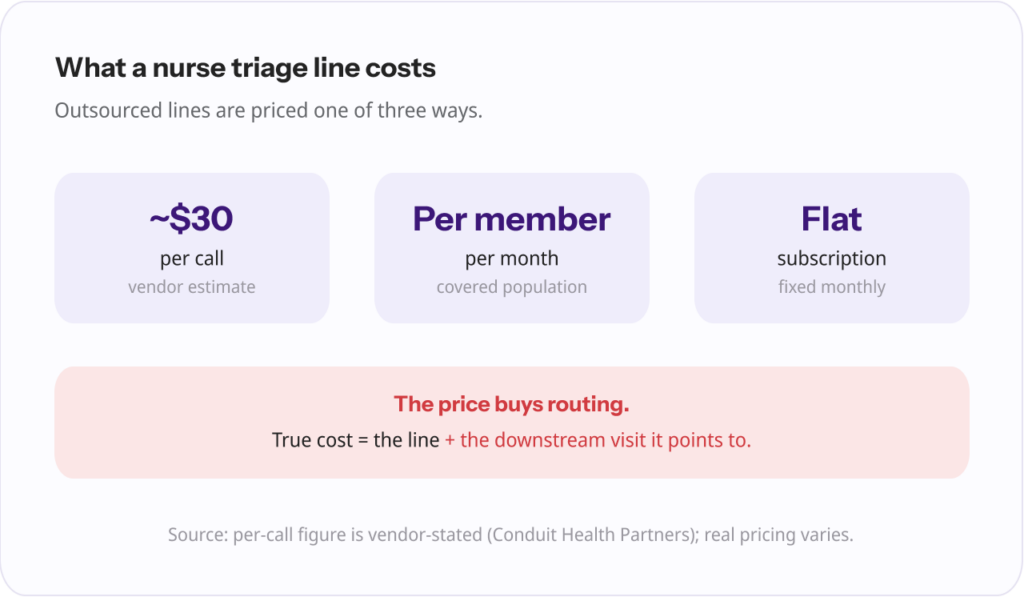
Outsourced lines are usually priced one of three ways: per call (a triage vendor estimates roughly $30 per call, though this is a vendor figure and real pricing varies), per member per month for a covered patient population, or a flat subscription.
In-house triage trades those per-call fees for fixed costs: nurse salaries for the hours you want covered, plus the software to guide them.
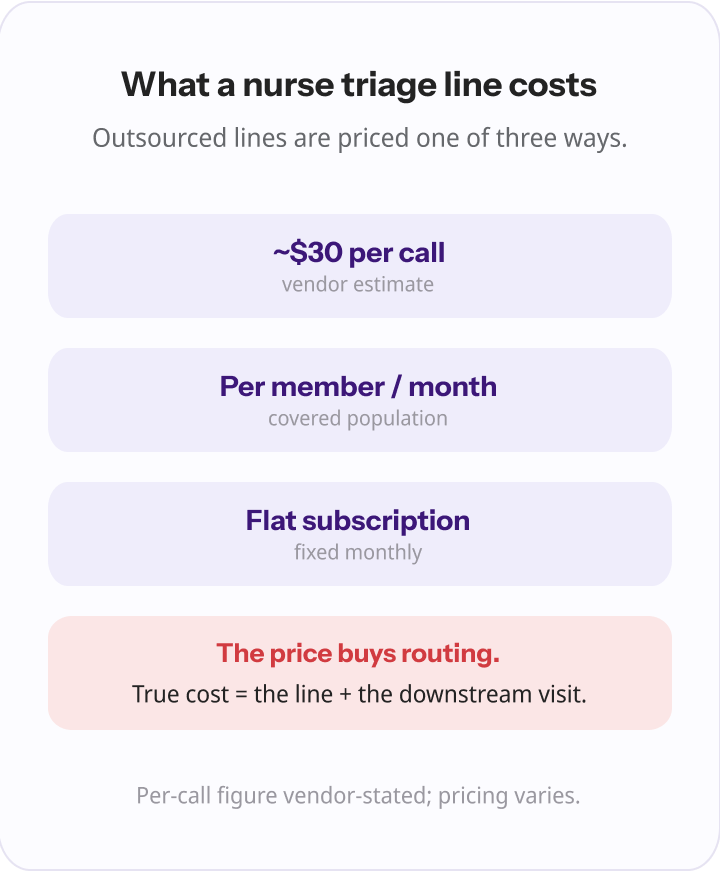
Here is the part to keep in front of you while you compare quotes. Whatever a nurse triage line costs, the price buys routing. The nurse tells the patient where to go. The care itself, the visit that actually treats the UTI or the ear infection, still has to happen somewhere, and you or the patient still pay for that separately.
So the true cost of a triage-only model is the line plus the downstream visit it points to. That framing matters for the comparison at the end of this guide.
If you do go the triage-line route, these are the criteria that actually separate a good service from a liability.
| What to look for | Why it matters |
|---|---|
| Standardized protocols (e.g., Schmitt-Thompson) | Consistent, defensible decisions instead of improvisation |
| Accreditation (e.g., URAC, which accredits health call centers) | An independent quality and safety standard you can verify |
| Documentation sent back to you | Continuity; you actually know what happened overnight |
| Genuine after-hours, weekend, and holiday coverage | This is the entire point, confirm the hours match your gaps |
| A clear escalation pathway | Emergencies and red flags get moved fast, not coached |
| Continuity (do patients stay attributed to you) | Protects the relationship and your downstream care |
| Whether it treats or only advises | Determines if the issue gets resolved or simply rerouted |
Most of these are table stakes a competent vendor will meet. The last row is the one practices skip, and it is the most important, because it is not really a feature comparison. It is a question about the model itself.
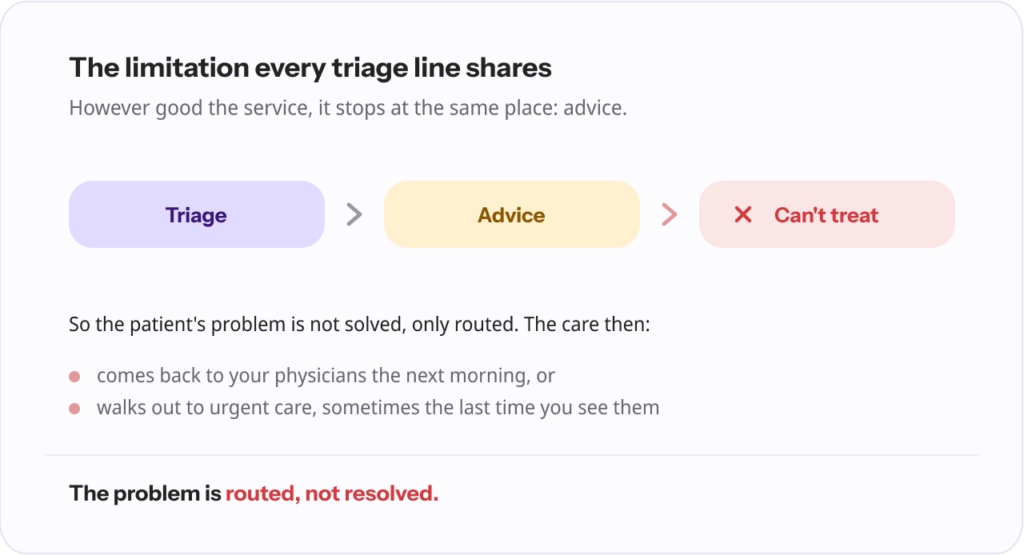
No matter how good the protocols are or how well the service is run, every nurse triage line, in-house or outsourced, stops at the same place: advice. A triage nurse cannot diagnose a condition or prescribe a medication.
That is not a knock on nurses or on any particular vendor; it is the defined scope of telephone triage. The nurse’s job is to assess and direct, full stop.

Which means the patient’s problem is not solved on that call. It is routed. The patient with a UTI at 9 p.m. is told to come in tomorrow or go to urgent care tonight, and then the actual treatment happens somewhere else, often back on your own physicians’ plates the next morning, or at the urgent care down the street, which is sometimes the last time you see that patient.
“Before a practice shops for a nurse triage line, I would ask them one question: do you want your after-hours calls routed, or resolved? A triage line routes. It is a real improvement over voicemail. But the nurse cannot treat the patient, so the work either comes back to your physicians in the morning or walks out the door to urgent care.” Ergo Sooru, Co-Founder & CEO, DrHouse.
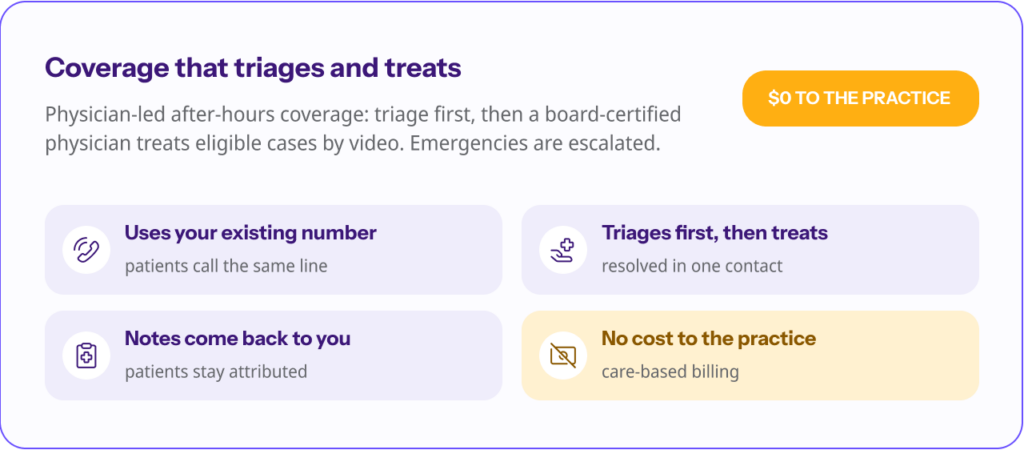
This is where a newer model has emerged: physician-led after-hours coverage that triages first, the same safe sorting step a nurse line provides, and then has a board-certified physician actually treat the eligible cases by video, prescribing when clinically appropriate and subject to physician judgment, patient eligibility, and applicable state laws. Emergencies are escalated rather than treated remotely.

The difference shows up clearly in a side-by-side.
| Nurse triage line | Physician-led after-hours coverage | |
|---|---|---|
| What it does | Advises and directs | Triages, then treats eligible cases |
| Can diagnose or prescribe | No | Yes, when clinically appropriate |
| Resolves the issue in one contact | No, care is deferred | Often yes |
| Cost to the practice | Per-call, per-member, or subscription | Can be $0 (care-based billing) |
| Patients stay attributed to you | Varies by service | Yes, with notes returned |
There is good evidence that adding a physician to the equation does more than resolve cases; it also keeps more patients out of the emergency room. In a U.S. Department of Veterans Affairs program, roughly two-thirds of patients a nurse line had steered toward the ER were safely redirected once a physician evaluated them, with no significant change in hospitalization or mortality.
And physician-led telemedicine is not the expensive option it sounds like: a 2026 Penn Medicine analysis of more than 163,000 visits found telemedicine cost roughly five times less per episode of care than in-person, without increasing short-term follow-up visits.
None of this makes a nurse triage line a bad choice. For some practices it is exactly right. But it does mean the decision is less “which triage line” and more “do I want routing or resolution,” and that is worth settling before you compare vendors.
“The thing that always struck me about the old model is that a practice pays a service to assess the patient and then hand the care right back, to your own team, or to the clinic down the street. You are paying to reroute your own after-hours burden. Coverage should remove the work and return the patient to you.” Ergo Sooru, Co-Founder & CEO, DrHouse.
If resolution is what you are after, it is worth seeing how physician-led after-hours coverage compares to a triage-only line, and we put the two head to head in our guide to nurse triage versus telehealth.
A nurse triage line is a real upgrade over a weekend voicemail. It gives anxious patients a clinician to talk to, keeps the worried-but-fine ones out of the ER, and protects your physicians’ nights.
If you choose one, weigh the things that matter, standardized protocols, accreditation, documentation back to you, true after-hours coverage, and a clean escalation path.
Just answer the bigger question first. A triage line tells your patients where to go. It does not treat them, which means the work, and sometimes the patient, ends up somewhere else.
If you would rather your after-hours calls came back to you resolved, with the patient still yours, a model that triages and treats is the one to look at.
A nurse triage line is a phone service, in-house or outsourced, where a registered nurse assesses a patient’s symptoms and advises on the right level and urgency of care. Practices use it to cover after-hours and overflow calls so patients reach a clinician instead of voicemail.
Outsourced lines are typically priced per call (a vendor estimate puts this around $30), per member per month, or by subscription. In-house triage trades per-call fees for nurse staffing and software costs. Remember that the price covers routing; the treatment the patient needs still happens, and is paid for, separately.
An answering service takes a message and passes it along. A nurse triage line adds clinical assessment: a registered nurse evaluates the symptoms and advises on the right level of care. Neither one treats the patient.
In-house gives you full control but requires staffing the overnight and weekend hours that are hardest to cover. Outsourcing hands off the staffing burden and provides built-in 24/7 coverage. Most small and mid-sized practices outsource the after-hours window because the demand is too thin to staff economically.
No. A triage nurse assesses and advises within the defined scope of telephone triage; they do not diagnose conditions or prescribe medication. Treatment requires a physician or other prescribing clinician, which is what physician-led after-hours coverage adds.
Standardized protocols (such as Schmitt-Thompson), independent accreditation, documentation returned to your practice, genuine after-hours and holiday coverage, a clear escalation pathway for emergencies, continuity so patients stay attributed to you, and whether the service treats patients or only advises them.
Content on the DrHouse website is written by our medical content team and reviewed by qualified MDs, PhDs, NPs, and PharmDs. We follow strict content creation guidelines to ensure accurate medical information. However, this content is for informational purposes only and not a substitute for professional medical advice, diagnosis, or treatment. For more information read our medical disclaimer.
Always consult with your physician or other qualified health providers about medical concerns. Never disregard professional medical advice or delay seeking it based on what you read on this website.
If you are experiencing high fever (>103F/39.4C), shortness of breath, difficulty breathing, chest pain, heart palpitations, abnormal bruising, abnormal bleeding, extreme fatigue, dizziness, new weakness or paralysis, difficulty with speech, confusion, extreme pain in any body part, or inability to remain hydrated or keep down fluids or feel you may have any other life-threatening condition, please go to the emergency department or call 911 immediately.
Experience 24/7 complete care in one visit, including treatment, prescriptions, and delivery.









on your schedule
Skip the unnecessary waiting room,
see a board-certified clinician now.
Prescriptions as needed
Renew or get a new Rx.
On-demand virtual visits
See a physician 24/7.
24/7 care support
We are here to help you.
Download the DrHouse app.
Set up your free account in a minute.
Start a visit with an online doctor. Wait time is less than 15 minutes.
Get an Rx from your preferred pharmacy. Pick up a Rx nearby or get it delivered to you.

on your schedule
Skip the unnecessary waiting room, see a board-certified physician now.
Available in 50 states. Insurance accepted.