|
Read time: 16 min
|
Posted on:
When you compare these two as after-hours coverage options, they aren’t doing the same job.
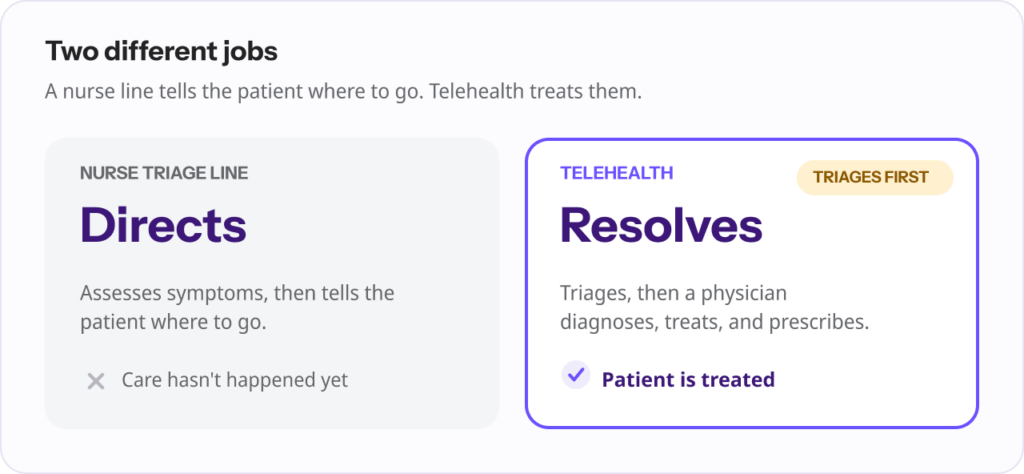
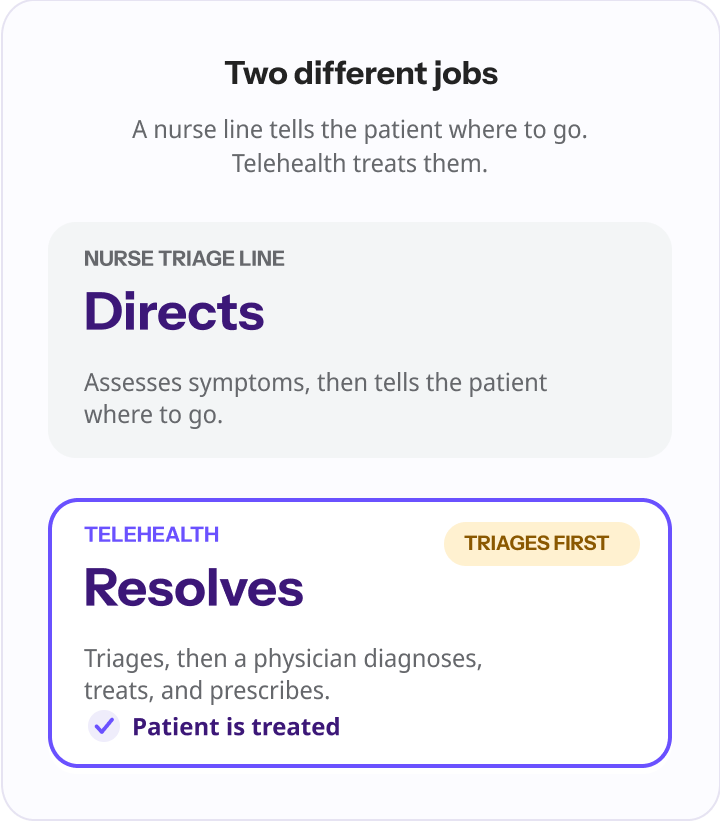
A nurse triage line directs the patient: it assesses symptoms and tells them where to go. Telehealth coverage resolves the patients needs: a physician diagnoses, treats, and prescribes when appropriate, and it triages first.
So the real question for a practice isn’t “triage or telehealth,” it’s whether your after-hours coverage should stop at telling patients where to go, or actually treat them. For most non-emergency after-hours care, coverage that triages and treats is the stronger choice.
It is 9 p.m. A patient calls with a urinary tract infection, or a parent calls about a feverish toddler. Your office is closed. What happens next is the entire ballgame for after-hours care, and practices generally choose between two models to handle it.
The first is a nurse triage line: a registered nurse answers, works through the symptoms, and tells the patient where to seek care. The second is telehealth coverage: the patient is triaged and then seen by a physician who can actually treat the problem.
Both are far better than voicemail. But they solve different problems, and understanding the difference is what lets you choose well.
This article compares them honestly, including where each falls short, and explains why, for after-hours non-emergency care, the model that triages and treats tends to win.
A nurse triage line is a disposition tool. A registered nurse assesses the caller’s symptoms using standardized decision-support protocols, most commonly the Schmitt-Thompson protocols, the widely used standard that covers roughly 350 pediatric and 400 adult topics (a figure stated by triage vendors).
Based on that assessment, the nurse assigns the safest next step: call 911, go to the ER now, go to urgent care, see your own provider tomorrow, or care for it at home.
Done well, this is genuinely valuable. It keeps worried patients out of the ER when they don’t need it, and it gets the sick ones to the right level of care quickly. The evidence supports its safety: a systematic review of remote triage commissioned by the Agency for Healthcare Research and Quality found that nurse-led telephone triage can be safe and broadly equivalent to physician triage for deciding where a patient should go.
Triage vendors report that 70 to 85% of calls are resolved without an ER visit, though those are industry figures rather than peer-reviewed results.
There is one hard limit, and it defines everything about the comparison: a triage nurse advises and directs, but does not diagnose or prescribe. When the call ends, the patient with a UTI still has a UTI. The care itself has not happened yet. It has been deferred to another visit, another contact, and often another bill.
“Triage answers one question: where should this patient go? That is genuinely useful at 2 a.m. It keeps people safe and out of the ER they don’t need. But it is not the same as fixing the problem. The patient with a UTI still has a UTI when the call ends. Telling someone where to get care and actually giving them care are two very different things.” Ergo Sooru, Co-Founder & CEO, DrHouse.
Telehealth coverage built for practices does not skip triage. It includes it, then goes one step further. The patient is triaged first, by intake and protocol, and eligible non-emergency cases are connected to a board-certified physician for a video visit.
The physician evaluates the patient, makes a diagnosis, treats the condition, and sends a prescription to the pharmacy when clinically appropriate, subject to physician judgment, patient eligibility, and applicable state laws. True emergencies and red-flag presentations are escalated.
The distinction that matters: a nurse line decides where care should happen, while telehealth coverage is the care. That is why the comparison is really triage-only versus triage-plus-treatment.
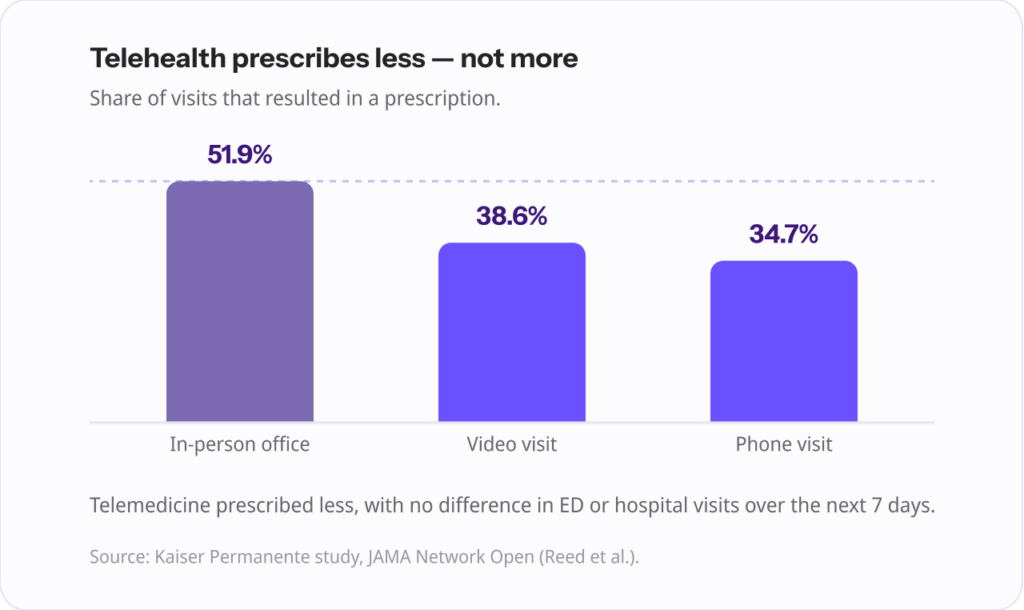
And the worry that telehealth physicians overprescribe or simply defer the problem does not hold up in the data. A Kaiser Permanente study published in JAMA Network Open found that a prescription was issued in 38.6% of video visits and 34.7% of telephone visits, compared with 51.9% of office visits.
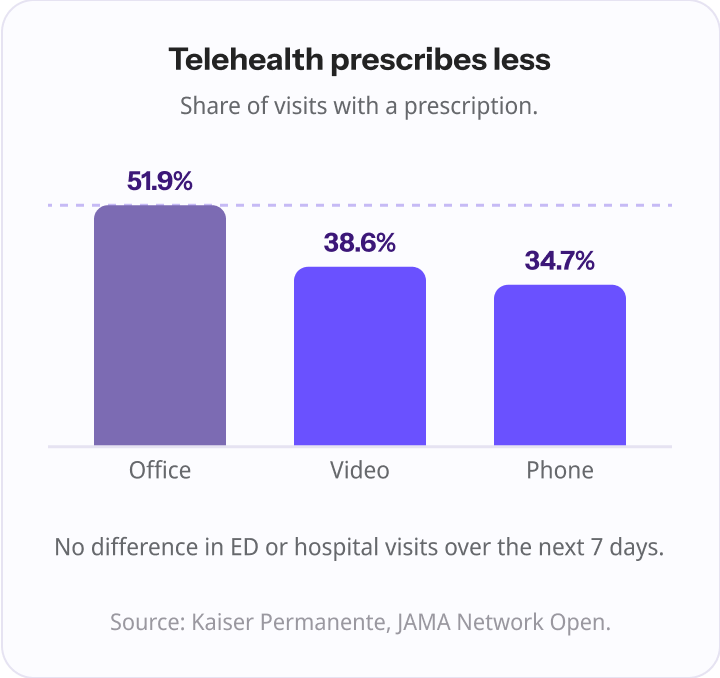
Telemedicine prescribed less, not more, with no difference in ED or hospital visits in the following seven days. In other words, physicians resolved cases appropriately rather than recklessly.
This is also where the health care system is heading. When the University of Pennsylvania health system recently moved to handle its after-hours primary care calls, it centralized them to a telemedicine service rather than a message-taking line.
Here is the core comparison, as a practice would actually weigh it.
| Nurse triage line | Telehealth coverage (physician-led) | |
|---|---|---|
| What it delivers | Advice and a disposition (where to go) | Triage plus actual treatment |
| Who handles the patient | Registered nurse | Triage, then a board-certified physician |
| Triage included | Yes | Yes |
| Can diagnose | No | Yes |
| Can treat and prescribe | No | Yes, when clinically appropriate |
| Resolves the issue in one contact | No, care is deferred | Often yes, for eligible cases |
| Diverts ED visits | Yes | Yes, and more of them safely |
| Cost to the practice | Per-call, per-member, or subscription | Can be $0 (care-based billing) |
| Continuity | Notes/disposition returned | Visit notes returned, patient stays attributed |
The three rows that matter most:
This is the single biggest difference. A nurse line ends with a recommendation. Telehealth coverage ends with a treated patient.
For the large share of after-hours calls that are routine acute issues (UTIs, sinus infections, pink eye, medication questions), the patient does not want a referral. They want to feel better.
Triage keeps people out of the ER, but adding a physician keeps even more of them out, safely. A U.S. Department of Veterans Affairs program that added physician tele-emergency evaluation to its nurse triage line found that roughly two-thirds of patients the nurses had triaged toward the ED were safely redirected once a physician assessed them, with no significant change in hospitalization or mortality.
Consistent with that, studies cited in the same research found physicians referred fewer callers to the ED than nurses did. For chest-pain callers, one study put it at about 10% (physicians) versus 16% (nurses); an England study found physicians sent only about 27% of would-be-ED callers on to the ED.
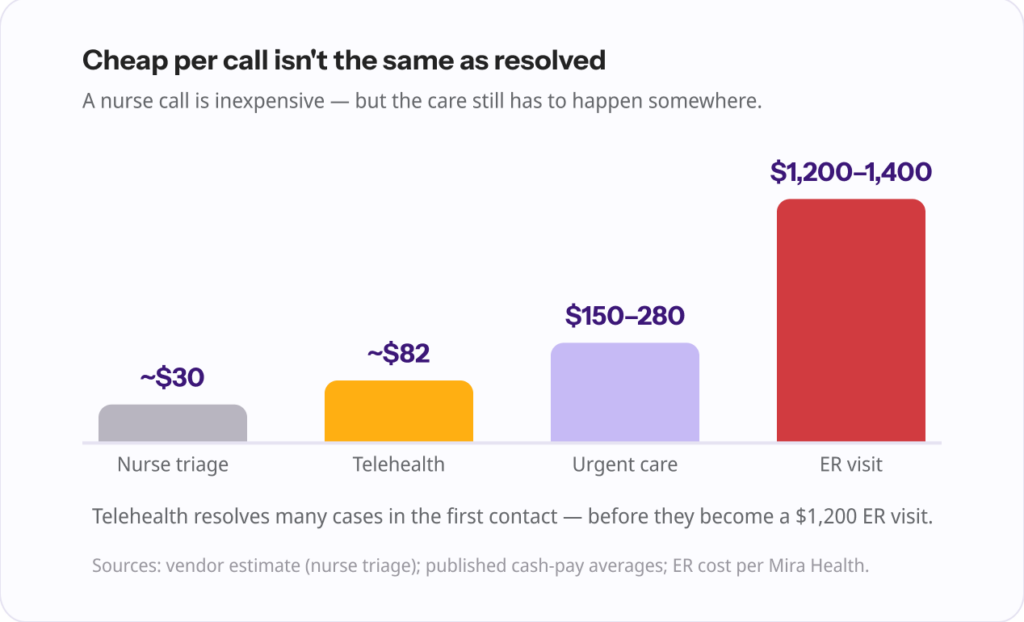
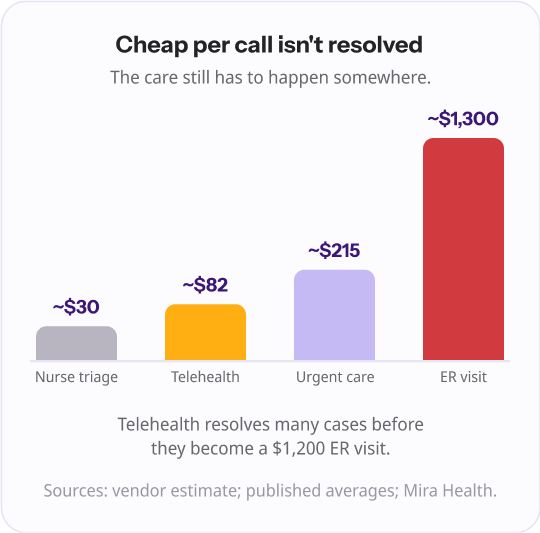
A nurse triage call is inexpensive on its own, around $30 per call by vendor estimates. But the practice pays for that line, and the actual care still has to happen somewhere, often the next day in your office, at urgent care ($150 to $280), or at the ED ($1,200 to $1,400, and an average of roughly $2,715 for the uninsured).
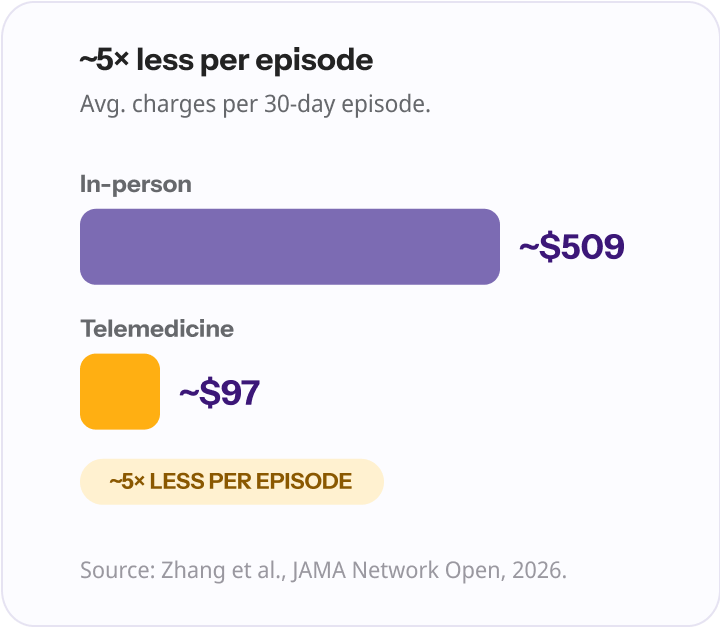
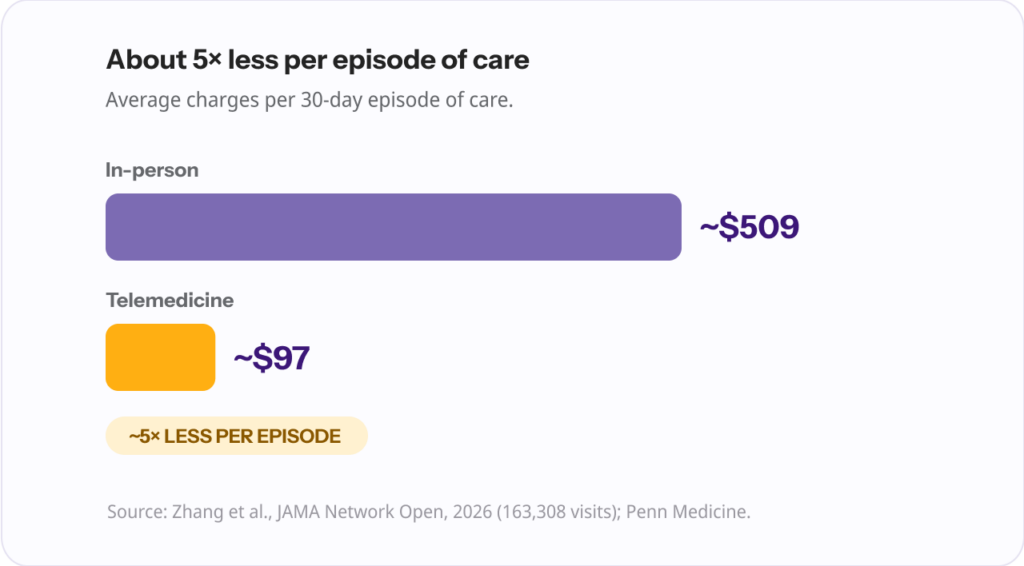
Telehealth resolves many of those cases in the first contact. A 2026 Penn Medicine analysis in JAMA Network Open of more than 163,000 visits found that telemedicine averaged about $97 in charges per 30-day episode of care versus about $509 for in-person, roughly five times less, without increasing short-term follow-up care.
Given that an estimated 71% of ED visits could be handled safely in a lower-acuity setting (a widely cited 2013 Truven analysis), resolving cases up front is where the real savings sit.
| Cost per contact, in context | Typical cost |
|---|---|
| Nurse triage call | ~$30 |
| Telehealth visit | $40 to $100 (median ~$82) |
| Urgent care visit | $150 to $280 |
| ED visit | $1,200 to $1,400 (uninsured avg ~$2,715) |
A fair comparison has to name the limits of both, because they are real and they shape the right answer.
Everything good about a nurse line ends at the recommendation. The patient still needs a second contact to actually resolve anything, which means deferred care, more steps, and a real chance the patient ends up at urgent care or the ER anyway, outside your practice.
Under-triage is the safety tail every triage program manages with red-flag protocols and conservative escalation thresholds.
Telehealth cannot perform a hands-on exam, and it is not appropriate for true emergencies or many complex presentations.
The evidence is not uniformly glowing, either: one JAMA Network Open cohort found that telehealth follow-up after an ED visit was associated with more repeat ED visits and admissions than in-person follow-up, on the order of 28 additional ED returns per 1,000 patients.
The lesson is not that telehealth is unsafe; it is that telehealth needs to triage first and escalate cleanly, rather than trying to be the answer to every call.
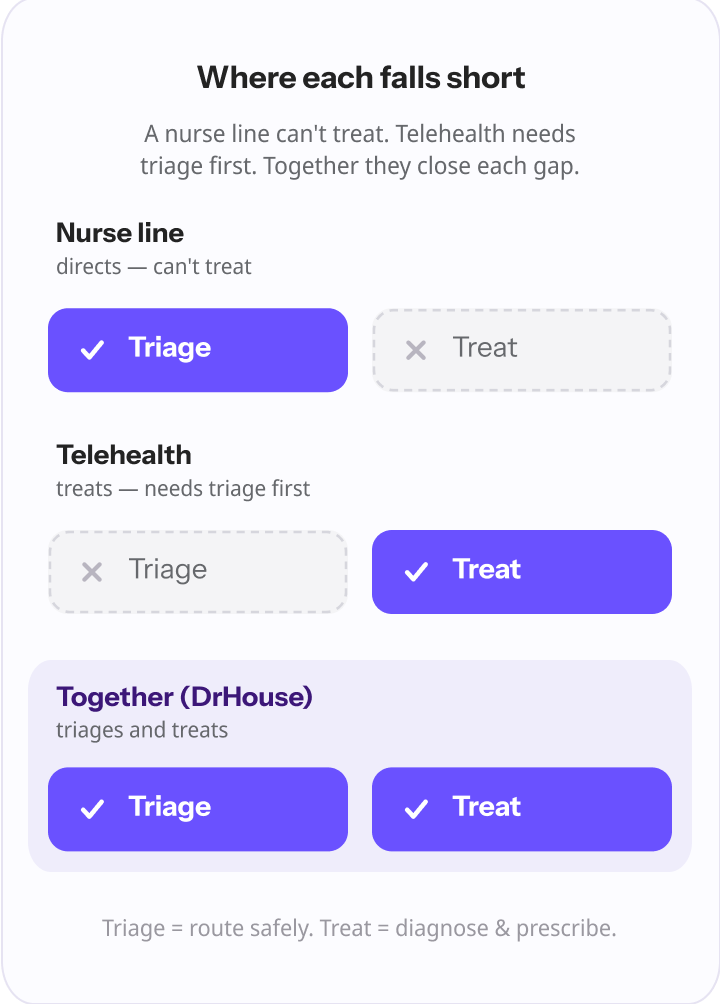
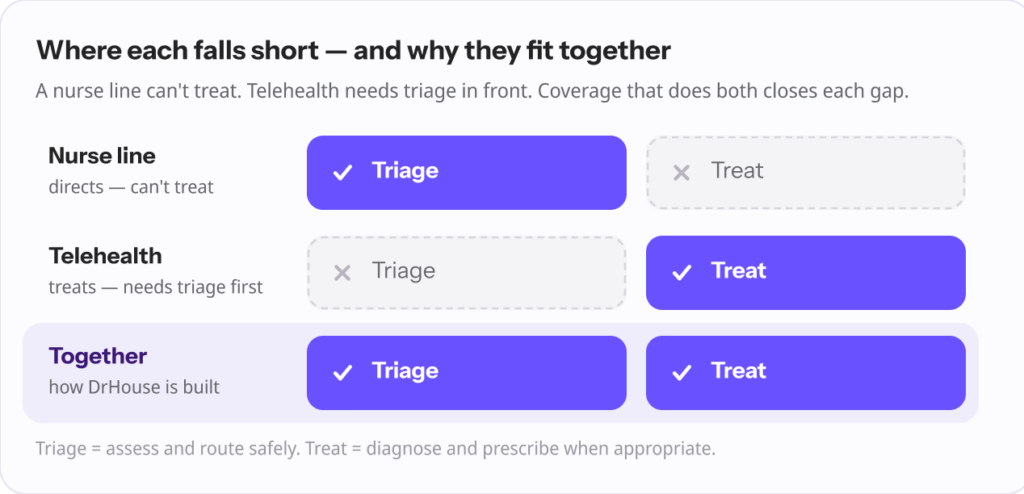
Notice that these failure modes are complementary. The nurse line’s weakness is that it stops before treatment. Telehealth’s weakness is that it needs strong triage and escalation in front of it. Put the two together and each covers the other’s gap.
This is the point that reframes the whole comparison. You do not actually have to choose between safe triage and real treatment, because good telehealth coverage already contains the triage.
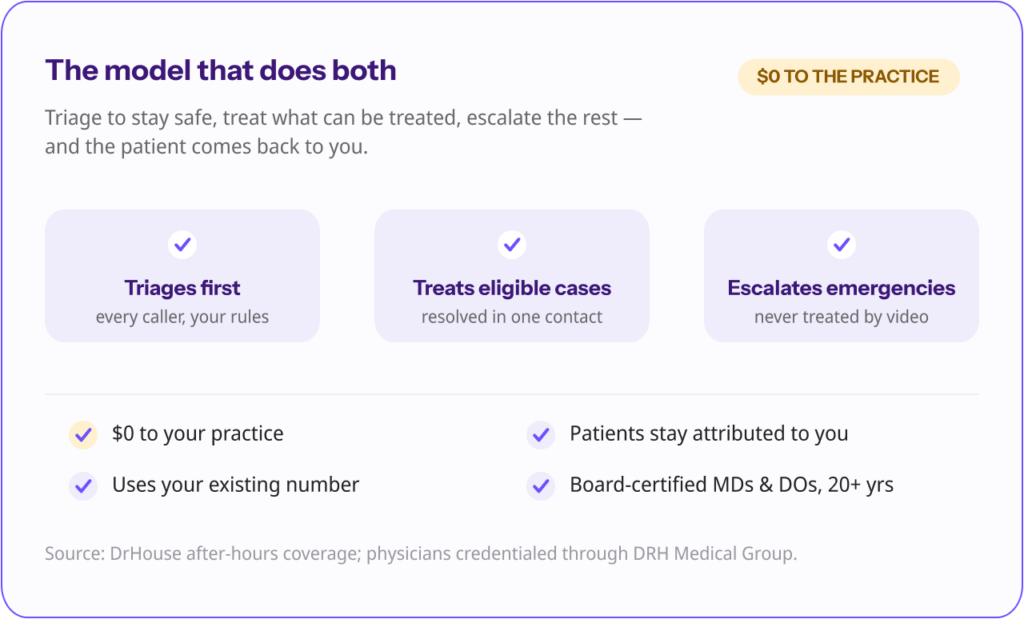
The strongest after-hours model triages every caller to stay safe, has a physician treat the cases that can be treated, and escalates the ones that cannot, then routes the documentation back to the practice.
That is how DrHouse is built. After-hours and overflow calls forward from your existing number. Patients complete a short AI-assisted intake and are triaged on rules your practice sets.
Eligible non-emergency cases are seen by a board-certified physician (licensed MDs and DOs credentialed through DRH Medical Group, with an average of more than 20 years of experience) who treats and prescribes when clinically appropriate.
Visit notes return to your practice by the next business day, and follow-ups route back to your team. Emergencies are escalated, not treated by video.
For a practice owner, the practical points are what separate this from a nurse line:
“For years practices were told to pick: a nurse line that points patients somewhere, or nothing. That was always a false choice. The patient calling after hours doesn’t want a referral, they want to feel better. The right model triages first to stay safe, then has a physician treat the cases that can be treated, and escalates the ones that can’t. You don’t have to choose between safe and resolved.” Ergo Sooru, Co-Founder & CEO, DrHouse.
“Here is the part that frustrates me about the old model: a practice pays a service to assess the patient and then hand the care right back to their own physicians, or send the patient out the door to urgent care. You are paying to reroute your own after-hours burden. Coverage should remove the work and return the patient to you, with notes, the next morning.” Ergo Sooru, Co-Founder & CEO, DrHouse
You can see how physician-led after-hours coverage that triages and treats compares to a message-and-disposition line in practice.
Run any option through these questions:
| Situation | Best-fit after-hours coverage | Why |
|---|---|---|
| Simple acute illness (UTI, sinusitis, pink eye) | Telehealth coverage | Can be diagnosed and treated in one contact |
| Medication or refill question | Telehealth coverage | A physician can act, not just advise |
| “Should I go to the ER?” reassurance | Either; telehealth adds treatment if needed | Both can triage; telehealth can also resolve |
| Possible emergency / red flags | Triage and escalate to ED or 911 | Neither model treats true emergencies |
| Complex or post-ED follow-up | In-person or practice’s own team | Telehealth is weaker here; needs hands-on care |
It was never really nurse triage versus telehealth as equals. A nurse triage line keeps patients safe and points them in the right direction, which matters, but it stops before the care happens.
Telehealth coverage triages and then treats, resolving most after-hours non-emergency cases in a single contact, diverting more ER visits safely, and keeping patients attributed to your practice.
For the after-hours calls that fill most practices’ nights and weekends, the coverage that triages and treats is the one that actually solves the patient’s problem, and yours. If that is the model you want, DrHouse provides it at no cost to the practice.
A nurse triage line assesses symptoms and tells the patient where to go (ER, urgent care, or home care), but the nurse does not diagnose or prescribe. Telehealth coverage triages the patient and then connects them to a physician who can diagnose, treat, and prescribe, resolving many cases in one contact.
No. Triage nurses advise and direct using standardized protocols. They do not diagnose conditions or prescribe medication. Treatment requires a physician or other prescribing clinician, which is what telehealth coverage adds.
Evidence suggests nurse-led telephone triage can be safe and broadly equivalent to physician triage for deciding where a patient should go, when it uses standardized protocols and conservative escalation. Safety depends on strong red-flag pathways for under-triage.
A nurse triage call is cheaper on its own (around $30 by vendor estimates), but the care still has to happen elsewhere, and the practice pays for the line. Telehealth resolves many cases in the first contact; a 2026 Penn Medicine study found telemedicine cost about five times less per episode of care than in-person. Care-based telehealth coverage can also be free to the practice.
Telehealth coverage built for practices already includes triage, so it does the nurse line’s job and adds treatment. It is not a replacement for emergency care; true emergencies are escalated rather than treated by video.
With DrHouse, no. The model is care-based, with patients billed for the care they receive, typically through insurance, so there are no setup fees, monthly costs, or per-call charges for the practice.
Content on the DrHouse website is written by our medical content team and reviewed by qualified MDs, PhDs, NPs, and PharmDs. We follow strict content creation guidelines to ensure accurate medical information. However, this content is for informational purposes only and not a substitute for professional medical advice, diagnosis, or treatment. For more information read our medical disclaimer.
Always consult with your physician or other qualified health providers about medical concerns. Never disregard professional medical advice or delay seeking it based on what you read on this website.
If you are experiencing high fever (>103F/39.4C), shortness of breath, difficulty breathing, chest pain, heart palpitations, abnormal bruising, abnormal bleeding, extreme fatigue, dizziness, new weakness or paralysis, difficulty with speech, confusion, extreme pain in any body part, or inability to remain hydrated or keep down fluids or feel you may have any other life-threatening condition, please go to the emergency department or call 911 immediately.
Experience 24/7 complete care in one visit, including treatment, prescriptions, and delivery.









on your schedule
Skip the unnecessary waiting room,
see a board-certified clinician now.
Prescriptions as needed
Renew or get a new Rx.
On-demand virtual visits
See a physician 24/7.
24/7 care support
We are here to help you.
Download the DrHouse app.
Set up your free account in a minute.
Start a visit with an online doctor. Wait time is less than 15 minutes.
Get an Rx from your preferred pharmacy. Pick up a Rx nearby or get it delivered to you.

on your schedule
Skip the unnecessary waiting room, see a board-certified physician now.
Available in 50 states. Insurance accepted.