|
Read time: 18 min
|
Posted on:
On-call duty is one of the most corrosive and overlooked drivers of physician burnout. You don’t fix it with resilience training, and you don’t need to hire your way out of it. The most effective lever is structural: move after-hours care (not just message-taking) off your own physicians entirely.
Below is the data behind the problem, the real cost of ignoring it, and how practices are solving it without adding headcount or cost.
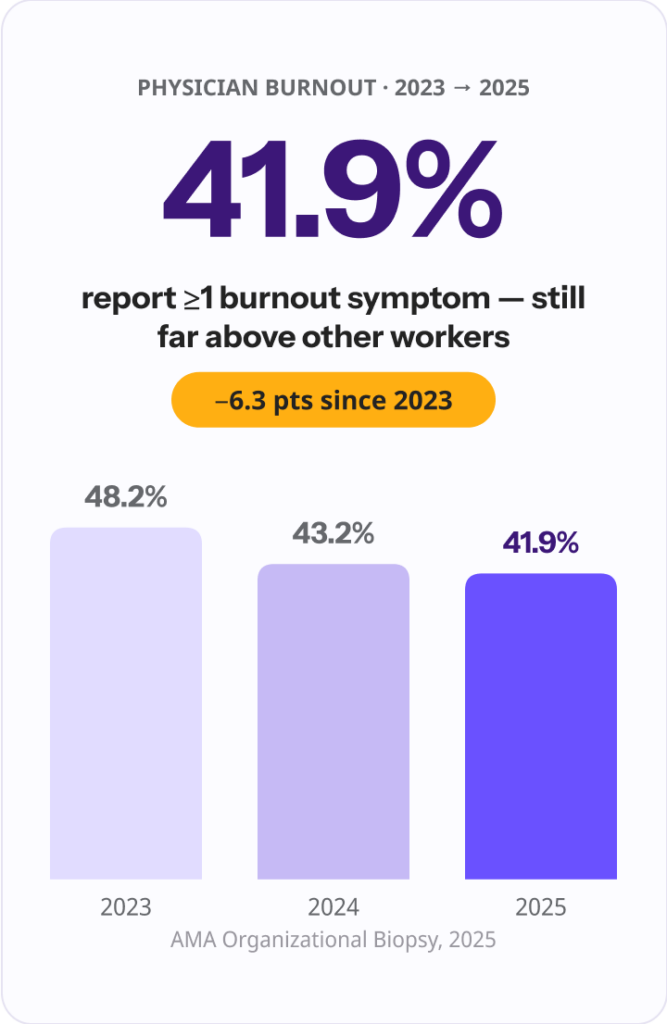
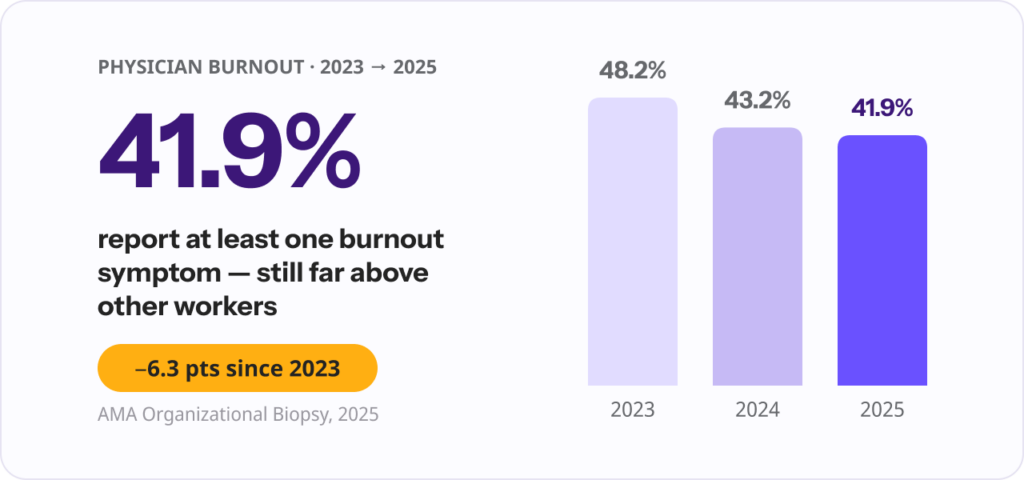
Burnout among U.S. physicians has eased slightly for four straight years, but it remains stubbornly high. According to the American Medical Association’s 2025 Organizational Biopsy, drawn from nearly 19,000 physicians across 106 health systems, 41.9% reported at least one symptom of burnout in 2025, down from 43.2% in 2024 and 48.2% in 2023.
A Stanford Medicine led study published in 2025 found that roughly half of physicians reported at least one symptom in late 2023 and early 2024. Even with the improvement, physician burnout sits well above that of the general working population.
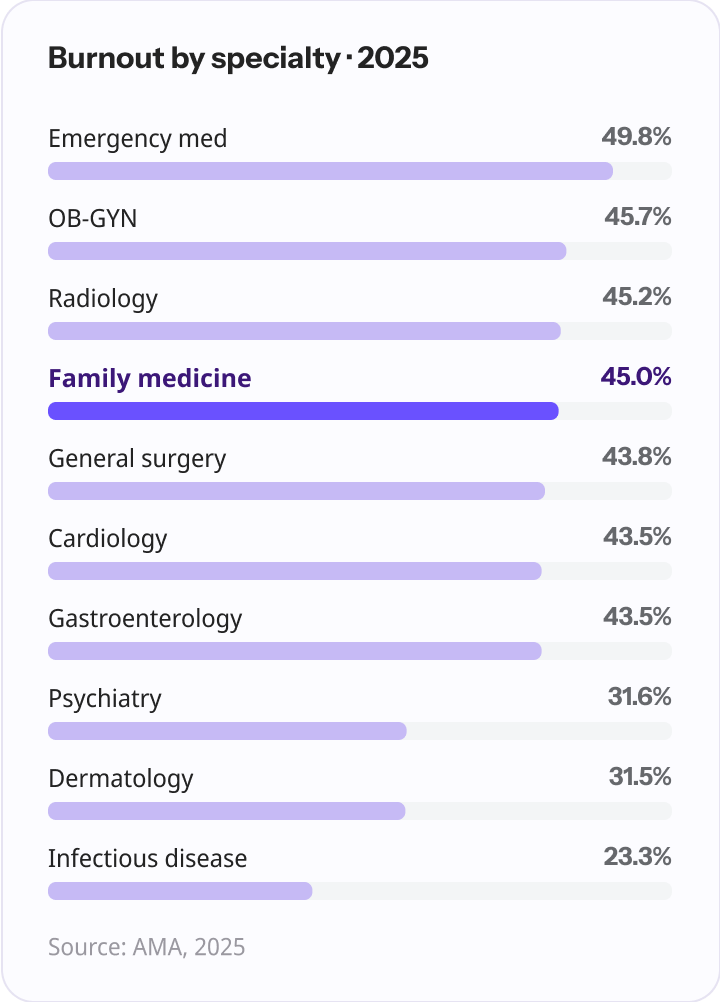
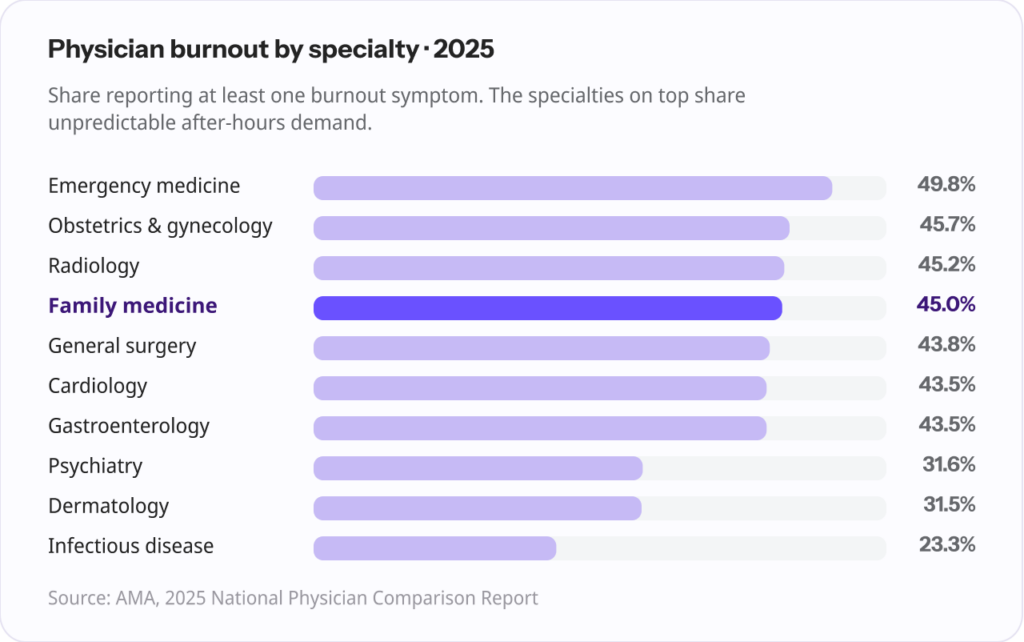
For primary care, the picture is sharper. Family medicine reported a 45% burnout rate in 2025, near the top of every specialty the AMA tracked.
| Specialty (2025) | Physicians reporting ≥1 burnout symptom |
|---|---|
| Emergency medicine | 49.8% |
| Obstetrics & gynecology | 45.7% |
| Radiology | 45.2% |
| Family medicine | 45.0% |
| General surgery | 43.8% |
| Cardiology | 43.5% |
| Gastroenterology | 43.5% |
| Psychiatry | 31.6% |
| Dermatology | 31.5% |
| Infectious disease | 23.3% |
Source: American Medical Association, 2025 National Physician Comparison Report.
The specialties at the top of that list share a common thread: unpredictable, after-hours demand. The mechanism by which on-call duty drives burnout is specific, and it’s worth understanding precisely, because it explains why the usual fixes miss.
A physician can work a long, full day and recover. What they don’t recover from easily is being woken at 2 a.m., handling a call, and being expected to function the next morning.
The American Academy of Sleep Medicine, in a position statement in the Journal of Clinical Sleep Medicine, identifies interrupted sleep while on call as a distinct risk factor for burnout, and reports that screening positive for a sleep disorder is associated with nearly four times the odds of burnout (odds ratio 3.78).
Field studies of physicians on night call have documented severely curtailed sleep, in some cases as little as three hours.
The problem compounds. Chronic partial sleep loss produces a dose-dependent decline in cognitive performance: research summarized in the BC Medical Journal found that getting under four hours of sleep per night for two weeks left subjects with cognitive ability comparable to two full nights of total sleep deprivation.
That’s not a one-bad-night problem. That’s the lived reality of a recurring call rotation.
The downstream effect on performance is well documented. In a study of pediatric residents cited by the BC Medical Journal, sustained attention and vigilance after an on-call shift were comparable to a blood-alcohol level between 0.04% and 0.05%. (That figure comes from resident, post-call research, but the underlying physiology of sleep deprivation isn’t unique to trainees.)
Add “sleep inertia,” the grogginess and impaired judgment that follow being jolted awake, and you have a clinician making decisions, then driving home, in a meaningfully degraded state.
Even when the phone doesn’t ring, the burden is there. Being on call means you can’t fully switch off, can’t be present with family, can’t recover.
Burnout researchers measure this through two of the core dimensions of the Maslach Burnout Inventory, emotional exhaustion and depersonalization, and a national analysis of physician task load found that the number of nights on call per week shows a dose-response relationship with both. More call nights, more exhaustion. It’s not a coincidence. It’s a gradient.
“The thing people miss about on-call is that the damage isn’t done by the calls you take. It’s done by the calls you’re waiting for. A physician who’s technically off but can’t sleep, can’t switch off, can’t be present with their family is still on the clock in every way that matters. That’s the part that wears people down.” Ergo Sooru, Co-Founder & CEO, DrHouse.
| What on-call does to a physician | What the evidence shows |
|---|---|
| Fragmented, insufficient sleep | Night-call sleep curtailed to as little as ~3 hours; interrupted sleep flagged as a distinct burnout risk factor. (Source: AASM position statement; J. Clin. Sleep Med.) |
| Higher burnout odds | Screening positive for a sleep disorder ≈ 3.78× the odds of burnout. (Source: AASM position statement) |
| Degraded performance post-call | Vigilance comparable to 0.04% to 0.05% blood-alcohol (resident data). (Source: BC Medical Journal, 2018) |
| Cumulative cognitive decline | Under 4 hrs/night for 2 weeks ≈ two nights of total sleep loss. (Source: BC Medical Journal, 2018) |
| Emotional exhaustion | Nights on call show a dose-response relationship with burnout. (Source: Physician Task Load national survey) |
For a practice owner or administrator, the clinical case for fixing this is also a financial one, and the numbers are larger than most expect.
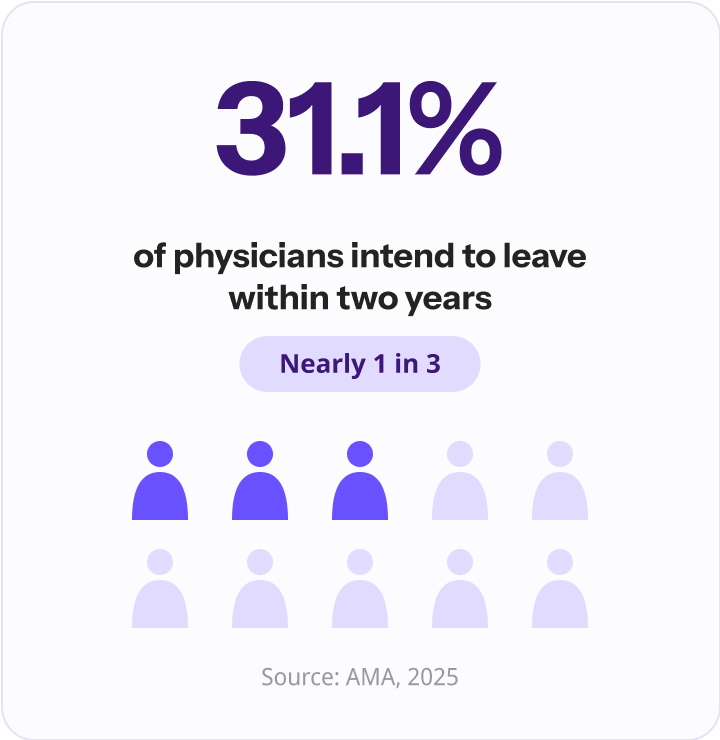
Burnout is the leading upstream driver of physician turnover. In the AMA’s 2025 data, 31.1% of physicians said they intended to leave their organization within two years. When one of them goes, the replacement cost is steep.
The AMA estimates that replacing a physician costs two to three times their annual salary, roughly $500,000 to more than $1 million per doctor once recruitment, sign-on bonuses, lost billings, and onboarding are counted. Stanford Medicine reported a floor of at least $250,000 per departure.
The costs don’t stop at recruitment. A study in Mayo Clinic Proceedings estimated that each primary care physician who leaves their practice generates about $86,336 in excess downstream health care expenditures the following year, as patients lose continuity of care.
Nationally, that analysis put burnout-related PCP turnover at roughly $260 million per year in excess spending.
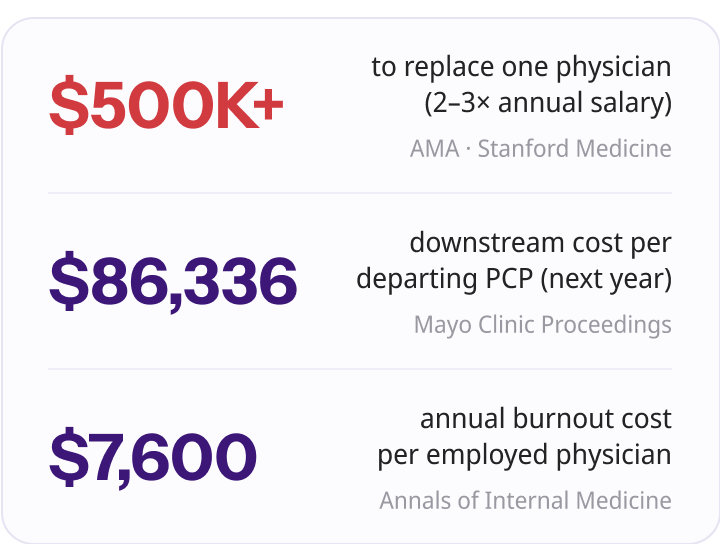
A separate, widely cited analysis in Annals of Internal Medicine placed the total annual cost of physician burnout in the U.S. at approximately $4.6 billion, or about $7,600 per employed physician, once reduced clinical hours are included.
| The cost of doing nothing | Estimated cost |
|---|---|
| Replacing one physician | $250,000 to $1,000,000+ |
| Downstream cost per departing PCP (following year) | ~$86,336 |
| Annual cost of burnout per employed physician | ~$7,600 |
Even on the conservative end, losing one physician you could have retained costs more than a year of most operational investments, and the on-call burden is one of the few drivers you can address structurally.
Replacement isn’t the only failure mode. Burnout often shows up first as a physician quietly cutting back: dropping to part-time, reducing panel size, or stepping away from call. That’s lost capacity a practice pays for without a resignation letter ever crossing the desk.
Practices that want to keep their physicians can shift the after-hours load off their own team entirely, which is covered below.
Most “physician burnout” advice is generic, and for on-call specifically, most of it doesn’t work. It’s worth being clear about why, because practices often try these first and conclude nothing helps.
Resilience training, mindfulness apps, and well-being webinars can support a physician, but none of them reduce the number of times the phone rings at night.
As the AMA and others have repeatedly noted, burnout is largely a function of the work environment, not individual coping capacity. Asking an exhausted physician to meditate harder doesn’t change the call volume.
This is the most important misconception to clear. A traditional medical answering service takes a message and routes it to the on-call physician. The physician is still woken, still calls the patient back, still makes a clinical decision, and still documents it in the morning.
The load isn’t eliminated. It’s shifted in time, often into the very overnight and early-morning hours that do the most damage. (For a deeper look at how these services actually operate, see our explainer on what a virtual medical answering service is and how it works.)
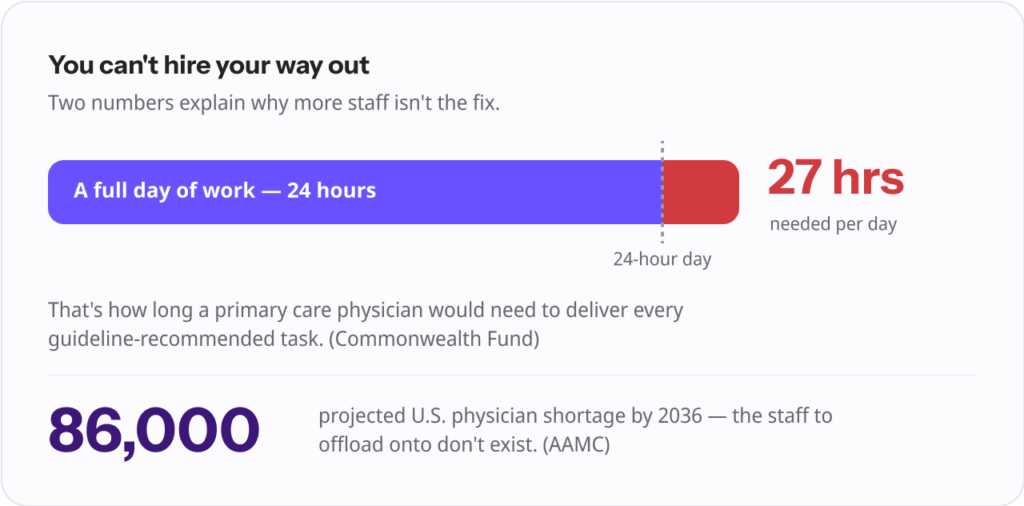
Adding a physician or bringing in locum coverage is the obvious answer, and often the wrong one for after-hours specifically. You’d be paying full clinical cost to cover a relatively thin band of overnight demand. It’s also swimming upstream: the Association of American Medical Colleges projects a U.S. shortage of up to 86,000 physicians by 2036.
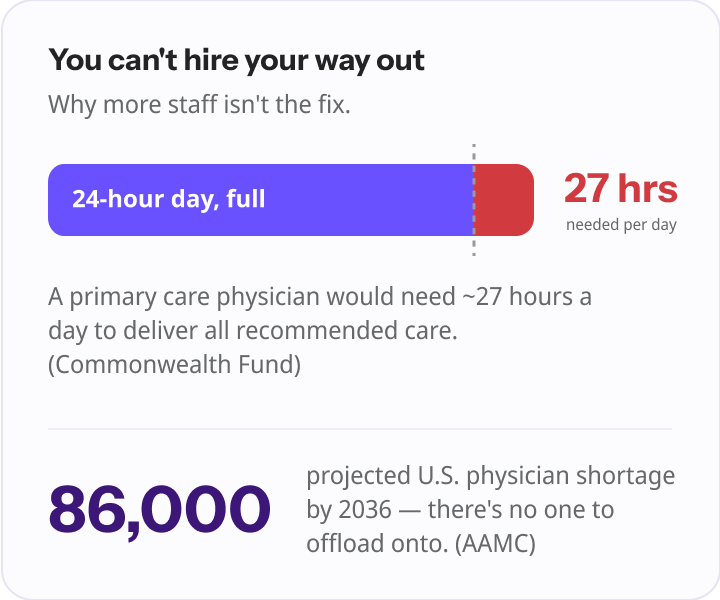
The Commonwealth Fund has illustrated the underlying squeeze starkly, estimating that a U.S. primary care physician would need nearly 27 hours in a day to deliver all recommended care and administrative work. There isn’t slack in the system to hire away an after-hours problem.
| Coverage model | Upfront cost | Ongoing cost | Physician load actually removed? | Continuity of care | Setup time |
|---|---|---|---|---|---|
| Keep call in-house | None | Physician time and burnout | No, it falls on your team | Full | None |
| Message-only answering service | Low | Per-call or monthly | No, work is deferred not removed | Full | Days |
| Locum or new hire | High | High (salary or locum rates) | Partial | Variable | Weeks to months |
| Physician-led after-hours telehealth | None | None to the practice | Yes, care handled externally | Full (notes return to you) | ~30 minutes |
There are real, incremental steps worth taking, and then there’s the structural change that does most of the work. Start with the first, but don’t stop there.
Level the load so no one physician absorbs the worst of it, make schedules predictable enough that physicians can plan recovery, and protect post-call time wherever possible. There’s evidence this matters: in one five-year cohort study, removing after-hours consult pager calls was among the interventions that meaningfully reduced strain.
“Pajama time,” clinical work done after hours, is one of the most persistent burnout drivers, and it isn’t improving. Per the AMA’s most recent data, 22.5% of physicians spend more than eight hours a week on the EHR outside normal working hours, up from 20.9% the year before.
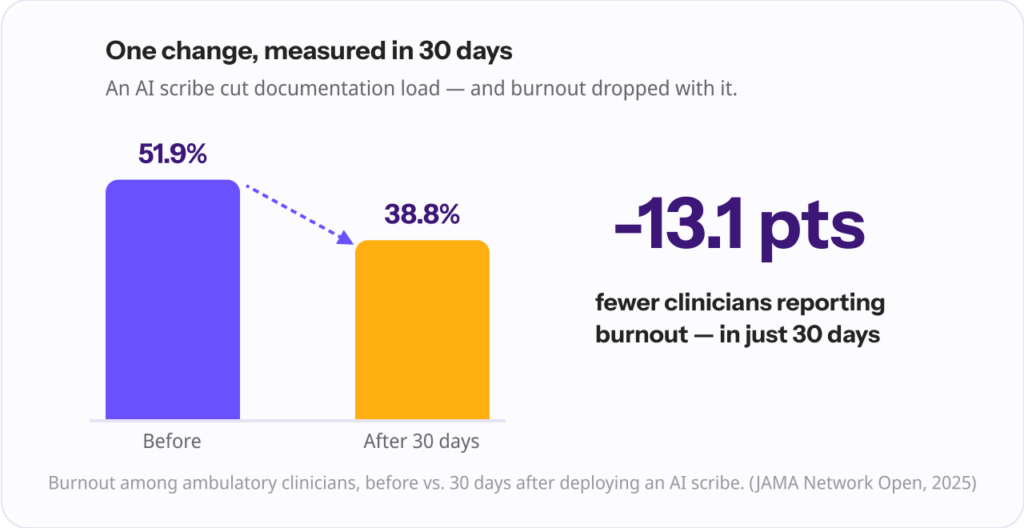
The after-hours documentation load isn’t shrinking. The encouraging news is that offloading administrative work demonstrably reduces burnout: a 2025 study in JAMA Network Open found that after 30 days using an ambient AI scribe, burnout among ambulatory clinicians fell from 51.9% to 38.8%, with measurable reductions in after-hours documentation time.
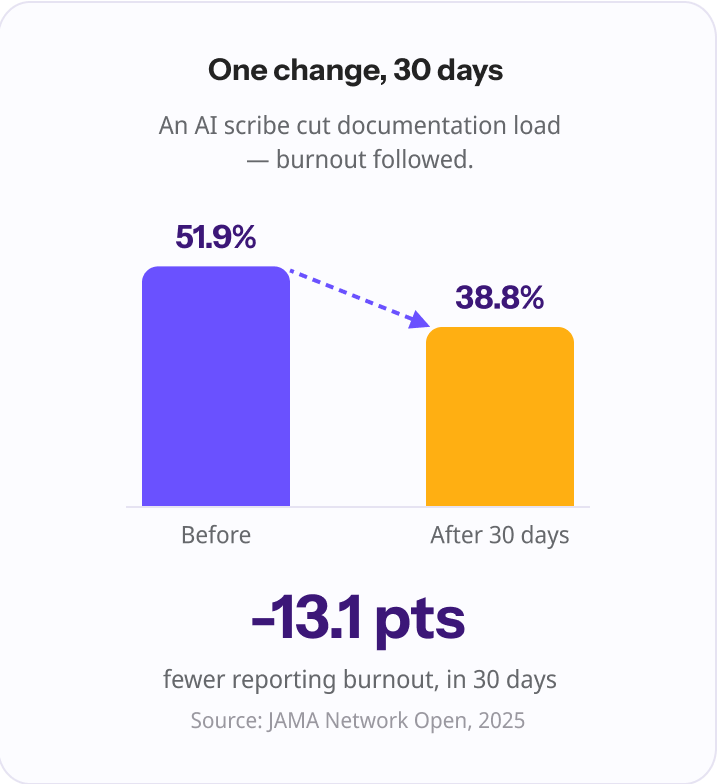
That’s a documentation intervention, not an on-call one, but it proves the principle: the lever that moves burnout is taking work away, not adding grit.
Much of after-hours volume is non-emergent and doesn’t require your physician personally. A structured intake that sorts true emergencies from routine concerns keeps the rotation focused on what actually needs them.
This is the structural fix, and it’s the one that removes load rather than relocating it. Instead of a service that wakes your physician to handle a call, board-certified physicians treat eligible after-hours, non-emergency cases directly, by video, and send the documentation back to your practice. Your own physicians aren’t paged. The work doesn’t pile up for the morning.
And critically, this can be done without adding a single hire.
“For decades the only options were to take the calls yourself or pay someone to take a message and hand the work right back to you. Neither one reduces the load. It just moves it around the clock. The shift we’re after is simple: when a non-emergency call comes in at night, an actual physician handles it, and your team wakes up to notes, not a backlog.” Ergo Sooru, Co-Founder & CEO, DrHouse.
The model that makes this work is straightforward, and it’s built to sit on top of how a practice already operates rather than asking it to change.
Patients call the practice’s existing number as they always have. After-hours and overflow calls forward automatically to a covering service, where patients complete a short AI-assisted intake and are triaged according to rules the practice sets.
For eligible cases, a board-certified physician conducts a video visit, evaluates and treats common non-emergency conditions, and, when clinically appropriate and subject to physician judgment, patient eligibility, and applicable state laws, sends prescriptions to the patient’s pharmacy.
Visit notes return to the practice by the next business day, and any follow-up needs route back to the practice’s own team.
With DrHouse, the physicians providing that care are licensed MDs and DOs, credentialed through DRH Medical Group, with an average of more than 20 years of clinical experience. The practical points that matter to a practice owner:
“Practices shouldn’t have to choose between protecting their physicians and protecting their patients, or take on new cost to do either. Coverage should extend the practice, not compete with it. The patients stay yours, the care comes back to you in the morning, and nobody has to be hired or paged to make it happen.” Ergo Sooru, Co-Founder & CEO, DrHouse.
This is the difference between deferring after-hours work and actually removing it, and it’s why physician-led after-hours coverage reduces the on-call burden in a way a message-taking service structurally cannot.
You don’t need a system overhaul to make progress. A practical sequence:
Step four is where most of the burnout reduction lives, and where moving after-hours care off your own team makes the largest difference.
Burnout from on-call duty isn’t a personal failing, and it isn’t an unavoidable cost of practicing medicine. It’s a design choice, and a fixable one.
The evidence is consistent: it’s driven by interrupted sleep and an always-reachable load, it’s expensive to ignore, and the interventions that actually move it are the ones that take work away from physicians.
You don’t need more people. You need the after-hours load to land somewhere other than on your own team. Practices that make that one structural change protect both their physicians and their patients, and increasingly, they’re doing it at no cost and with no new hires.
Level the call load across physicians, keep schedules predictable, protect post-call recovery time, and, most effectively, reduce how many after-hours calls reach a physician at all. Routing non-emergency after-hours care to a covering physician-led service removes the load rather than redistributing it among your own team.
Yes. Much of the on-call burden is non-emergent volume that doesn’t require your own physicians personally. Offloading that after-hours care to board-certified physicians externally reduces strain without adding headcount, and avoids paying full clinical cost to cover a thin band of overnight demand.
With DrHouse, no. The model is care-based: patients are billed for the care they receive, typically through insurance. There are no setup fees, no monthly costs, and no added overhead for the practice.
Yes. Patients remain fully attributed to your practice. All follow-ups and ongoing care route back to your team, and visit notes are returned to you, typically by the next business day, so continuity is preserved.
A message-only answering service takes a message and hands the work back to your on-call physician, who is still woken and still owes documentation. Physician-led after-hours coverage has a board-certified physician actually treat the patient and return notes to you, so the work is removed, not deferred.
Because it works with a practice’s existing phone number and requires no new software, many practices can begin routing after-hours calls in about 30 minutes, once call forwarding and triage preferences are confirmed.
Content on the DrHouse website is written by our medical content team and reviewed by qualified MDs, PhDs, NPs, and PharmDs. We follow strict content creation guidelines to ensure accurate medical information. However, this content is for informational purposes only and not a substitute for professional medical advice, diagnosis, or treatment. For more information read our medical disclaimer.
Always consult with your physician or other qualified health providers about medical concerns. Never disregard professional medical advice or delay seeking it based on what you read on this website.
If you are experiencing high fever (>103F/39.4C), shortness of breath, difficulty breathing, chest pain, heart palpitations, abnormal bruising, abnormal bleeding, extreme fatigue, dizziness, new weakness or paralysis, difficulty with speech, confusion, extreme pain in any body part, or inability to remain hydrated or keep down fluids or feel you may have any other life-threatening condition, please go to the emergency department or call 911 immediately.
Experience 24/7 complete care in one visit, including treatment, prescriptions, and delivery.









on your schedule
Skip the unnecessary waiting room,
see a board-certified clinician now.
Prescriptions as needed
Renew or get a new Rx.
On-demand virtual visits
See a physician 24/7.
24/7 care support
We are here to help you.
Download the DrHouse app.
Set up your free account in a minute.
Start a visit with an online doctor. Wait time is less than 15 minutes.
Get an Rx from your preferred pharmacy. Pick up a Rx nearby or get it delivered to you.

on your schedule
Skip the unnecessary waiting room, see a board-certified physician now.
Available in 50 states. Insurance accepted.